Download
1 / 61
780 likes | 1.82k Vues
Clinical Overview of Age-Related Macular Degeneration. Victor H. Gonzalez, MD Medical Director Valley Retina Institute McAllen, TX. Age-Related Macular Degeneration. Affects patients ≥ 50 years of age Caucasian race, cigarette smoking, obesity, and hypertension are significant risk factors

E N D
Clinical Overview of Age-Related Macular Degeneration Victor H. Gonzalez, MD Medical Director Valley Retina Institute McAllen, TX
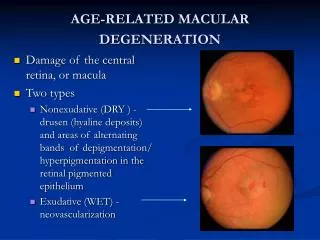
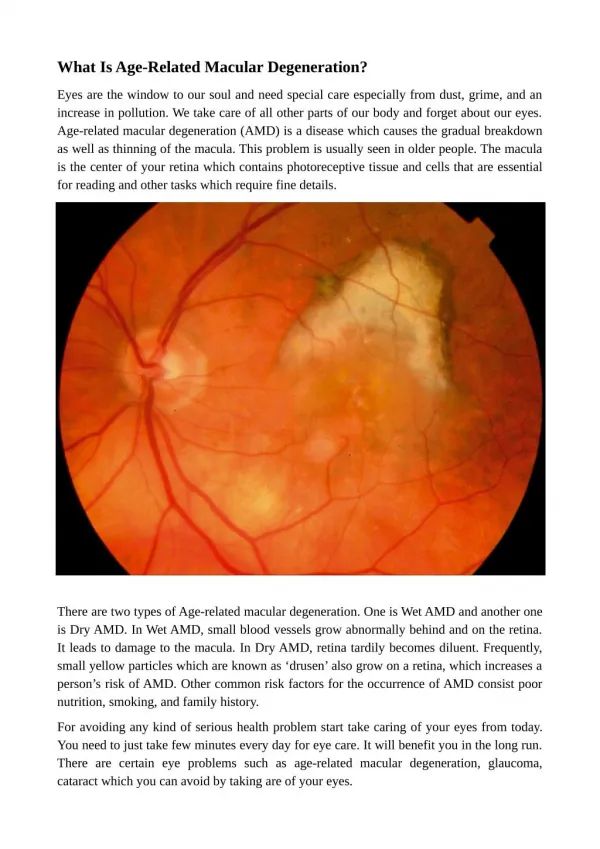
Age-Related Macular Degeneration • Affects patients ≥ 50 years of age • Caucasian race, cigarette smoking, obesity, and hypertension are significant risk factors • Condition marked by the appearance of drusen, an accumulation of apparently undigested products of retinal pigment epithelial cells under the basal lamina of Bruch's membrane • Progressive deterioration of Bruch’s membrane, the retinal pigment epithelium, choriocapillaris, and outer retina in the macular area
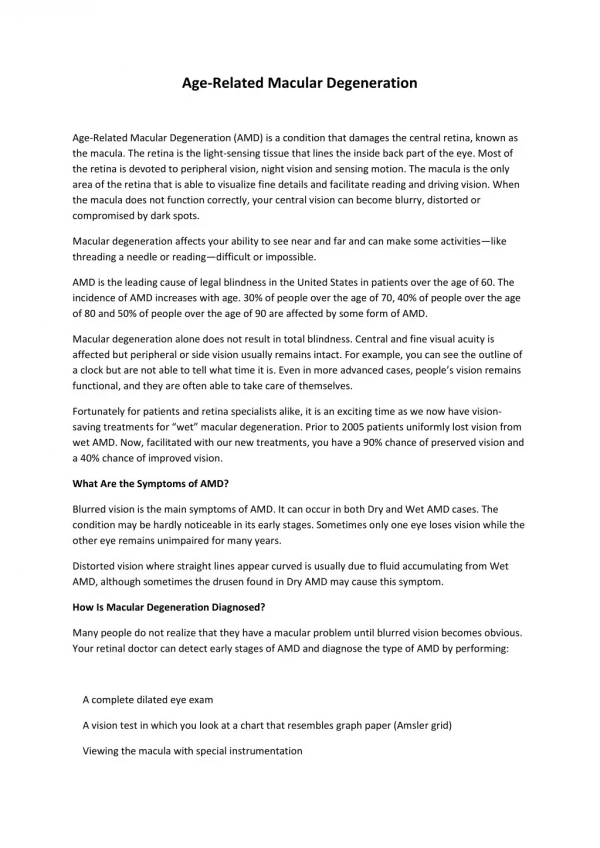
Age-Related Macular Degeneration (AMD) • Leading cause of severe vision loss in the developed countries • Marked by • Decreased visual acuity and contrast sensitivity • Metamorphopsia and scotoma • 2 forms • Non-neovascular (dry) • Neovascular (exudative, or “wet”) • 90% of severe vision loss results from wet AMD Vingerling JR. Epidemiol Rev. 1995;17:347. Hyman L. Age Related Macular Degeneration: Principles and Practice. New York: Raven Press; 1992;1-32.
Age-Related Macular Degeneration (AMD) Advanced AMD (choroidal neovascularization or central GA) currently affects approximately 1.4 million people in the United States. • ~ 8 million Americans at high risk for developing advanced AMD • Potential increase in cases to 3 million by year 2020 GA = Geographic atrophy. Friedman DS, et al. Arch Ophthalmol. 2004;122:564-572. Bressler NM, et al. Arch Ophthalmol. 2003:121:1621-1624.
Drusen and AMD—Progression Drusen Hemorrhagic Detachment RPE & Sensory Detachment RPE Atrophy Fibrous Disciform Scar Exudative AMD Dry AMD RPE = retinal pigment epithelium. Jack J. Kanski, Jay Menon. Clinical Ophthalmology:A Systematic Approach. Elsevier Science; 2003.
How Is AMD Detected? • Clinical exam • Visual function measurement • Visual acuity • Amsler grid • Contrast sensitivity • Diagnostic procedures • Fluorescein angiography • Optical coherence tomography 1 2 2 1. http://images.google.com/images?q=Amsler+grid+%2B+AMD&ndsp=20&svnum=10&hl=en&lr=&client=firefox-a&rls=org.mozilla:en-US:official_s&start=0&sa=N 2. Image courtesy of Dr. V. Gonzalez, Valley Retina Institute P.A.
Interventions to Slow Progression • AREDS formulation • Vitamin C 500 mg • Vitamin E 400 IU (400 mg) • Beta-carotene 15 mg (28640 IU vitamin A) • Zinc oxide 80 mg • Cupric oxide 2 mg • Principal finding of study • Antioxidant vitamin/mineral (zinc) supplements modestly reduced risk of progression and vision loss over 6 years vs placebo AREDS = Age-Related Eye Disease Study. AREDS Research Group. Arch Ophthalmol. 2001;119:1417.
AREDS Summary • Early AMD • No benefit from supplements • Intermediate AMD/monocular advanced AMD • Antioxidants plus zinc or zinc alone significantly reduced the risk of developing advanced AMD • An estimated 300,000 Americans could avoid developing advanced AMD over 5 years by taking AREDS-type supplements AREDS Research Group. Arch Ophthalmol. 2001;119:1417.
Wet AMD • Less common than dry AMD, but more serious • 90% of severe vision loss results from wet AMD • Metamorphopsia is the initial symptom. Most lesions are not visible clinically Hyman L. Age Related Macular Degeneration: Principles and Practice. New York: Raven Press; 1992. Image courtesy of Dr. V. Gonzalez, Valley Retina Institute P.A.
Treatments for Wet AMD • Thermal laser coagulation1 • MPS: Macular Photocoagulation Study • Photodynamic therapy with verteporfin • TAP: Treatment of Age-Related Macular Degeneration with Photodynamic therapy2 • VIP: Verteporfin in Photodynamic therapy3 • Anti-VEGF therapies • Pegaptanib sodium • VISION: VEGF Inhibition Study in Ocular Neovascularization4 • Ranibizumab (Lucentis) • ANCHOR Trial5MARINA Trial6 FOCUS Trial7 • Bevacizumab (Off-label)8 1. Macular Photocoagulation Study Group. Arch Ophthalmol. 1994;112:500. 2. (TAP) Study Group. Arch Ophthalmol. 1999; 117:1329. 3. VIP Study Group. Am J Ophthalmol. 2001;131:541. 4. Gonzales CR. Retina. 2005;25:815. 5. ANCHOR Study Group. Invest Ophthalmol Vis Sci. 2006;47:E-Abstract 2963. 6. MARINA Study Group. Invest Ophthalmol Vis Sci. 2006; 47:E-Abstract 2959. 7. http://www.gene.com/gene/news/press-releases/display.do?method=detail&id=9147. 8. http://www.fda.gov/CDER/foi/label/2004/125085lbl.pdf#search=%22Avastin%20package%20insert%22.
Laser Photocoagulation • Obliterates choroidal neovascularization (CNV), preventing further growth of fibrovascular tissue • For some patients, it remains the 1st-line therapy for well demarcated extrafoveal/juxtafoveal CNV lesions • 50% chance of recurrence within 2 years of treatment • May damage surrounding tissue Macular Photocoagulation Study Group. Arch Ophthalmol. 1991;109:1220. Fine SL, et al. N Engl J Med. 2000;342:483.
Photodynamic Therapy with Verteporfin Photodynamic therapy • Rapid closure of vessels • Intra- and extracellular infiltration of inflammatory cells • Increased edema in the short term • Transient antiangiogenic effects • Upregulates vascular endothelial growth factor • 90% of patients need retreatment at 3 months Schmidt-Erfurth U, et al. Invest Ophthalmol Vis Sci. 2002;43:830.
Photodynamic Therapy Studies • TAP Study1 • Multicenter, double-blind, placebo-controlled, randomized, clinical trial of verteporfin vs placebo • AMD with classic subfoveal lesions • Significant benefit with PDT therapy at 12 and 24 months • VIP Study2 • Occult or minimally classic • By month 24, verteporfin group was less likely to have moderate to severe vision loss TAP = Treatment of age-related macular degeneration with photodynamic therapy; PDT = photodynamic therapy; VIP = Verteporfin In photodynamic therapy 1. TAP Study Group. Arch Ophthalmol. 1999;117:1329. 2. VIP Study Group. Am J Ophthalmol. 2001;131:541.
Vascular Endothelial Growth Factor1 • A protein that regulates angiogenesis (normal and abnormal) • Member of a family of angiogenic and lymphangiogenic growth factors • Secreted by a variety of cells in response to hypoxia/ischemia and other signals • Many strategies now target this factor2 • Interfering with pro-angiogenic growth factors, receptors, or downstream signaling • Upregulating endogenous inhibitors, or administering exogenous inhibitors • Directly targeting neovasculature 1. Adamis AP, et al. Retina. 2005;25:111. 2. Witmer AN, et al. Prog Retin Eye Res. 2003;22:1.
Pegaptanib—Anti-VEGF Aptamer Selective VEGF inhibition • Binds selectively to VEGF165 • Pathologic isoform • Spares normal vasculature • Mechanisms of action • Antiangiogenic2 • Antipermeable2 • Antiinflammatory3 Pegaptanib 1 Pegaptanibbinds to VEGF165 VEGF = vascular endothelial growth factor 1. http://www.revophth.com/index.asp?page=1_652.htm. 2. Ishida S, et al. J Exp Med. 2003;198:483. 3. Carrasquillo KG , et al. Invest Ophthalmol Vis Sci. 2003;44(1):290.
VEGF Inhibition Study in Ocular Neovascularization (VISION) • Two randomized controlled studies involving 1186 patients in 117 centers • Intravitreal injections every 6 weeks for 1 year • Primary endpoint: % of patients losing <15 letters at 1 year • Mean letters of visual acuity loss: 8 in pegaptanib-treated vs 15 in placebo at 1 year Gragoudas ES. N Engl J Med. 2004;351:2805.
VISION Study Primary efficacy endpoint: % of patients losing <15 letters at week 54 Adapted with permission from Gragoudas ES. N Engl J Med. 2004;351:2805. Copyright © 2004 Massachusetts Medical Society. All rights reserved.
Ranibizumab • Humanized fragment of a monoclonal antibody • Targets all isoforms of VEGF • 3 randomized clinical trials (ANCHOR, MARINA, and FOCUS) Ranibizumab Genentech, Inc. Data on file.
RanibizumabANCHOR Trial • 423 patients with predominantly classic CNV randomized to • PDT/sham injection Q 3 mo for 2 years • Placebo PDT/0.3 mg ranibizumab injection once per month • Placebo PDT/0.5 mg ranibizumab injection once per month1 • Primary endpoint: % of patients losing <15 letters in 1 year1 • Endpoint reached by 94% and 96% of patients • Vision improved in 36% – 40% of patients2 CNV = choroidal neovascularization; PDT = photodynamic therapy 1. Kaiser PK. Ophthalmology. 2005;9(1). 2. http://www.clinicaltrials.gov/ct/show/NCT00061594?order=3.
RanibizumabMARINA Trial • 716 patients with minimally classic or occult lesions • Patients randomized to monthly injections with 0.3 mg or 0.5 mg ranibizumab, or sham • Therapy found to improve vision in patients with wet AMD Association for Research in Vision and Ophthalmology. ARVO2006. 2006.
MARINA Year 1 Resultsand Conclusions • 95% of ranibizumab subjects lost <15 letters (vs 62% of sham) • 25% – 34% of ranibizumab subjects gained ≥15 letters (vs 5% of sham) • First phase III clinical trial to show improvement in mean visual acuity • No serious ocular side effects • No apparent systemic safety concerns Association for Research in Vision and Ophthalmology. ARVO2006. 2006.
Bevacizumab (Off-Label) • Recombinant humanized monoclonal antibody that binds VEGF • First anti-VEGF medication FDA approved as treatment for metastatic colorectal cancer • Not approved for ophthalmic use • Demonstrated efficacy in 2 case series (50 and 79 patients)1,2 1. Rich RM, et al. Retina. 2006;26:495. 2. Avery RL, et al. Ophthalmology. 2006;113:363.
AMD Summary • AREDS formulation significantly reduces the risk of progression from intermediate to advanced AMD1 • Pegaptanib sodium provides a safe treatment for all lesion compositions2 • Recently approved ranibizumab is the first drug to improve visual acuity in 30% – 40% of patients3 1. AREDS Research Group. AREDS report no. 8. Arch Ophthalmol. 2001;119:1417. 2. D’Amico DJ, et al. Clinical Trial Group. Ophthalmology. 2006;113:1001. 3. Heier JS, et al. Ophthalmology. 2006;113:642.
Treatment Summary • Early data suggest that anti-VEGF treatment alone may not be a long-term solution • Numerous other antiangiogenic and/or anti- inflammatory agents offer hope for the future • – Bevacizumab • – Anecortave acetate • – Triamcinolone acetonide • – VEGF trap • – siRNAs • – Squalamine lactate • – Kinase inhibitors • – AdPEDF
The Goals of Treating AMD • To minimize loss of visual acuity and central vision • To preserve reading ability with/without visual aids • To optimize quality of life • To minimize adverse effects of treatment modalities
We look forward to the next decade of AMD management, as investigations on antiangiogenesis, inflammation, and other strategies continue.
Health-Related Quality of Life and Health Economics Associated with AMD Glenda S. Owens, RPh, MHA, CDM Vice President Pharmacy Services Arcadian Health Plan San Dimas, California
Burden of Age-Related Macular Degeneration (AMD) and Visual Impairment • AMD is the most common cause of severe, irreversible vision loss • An estimated 200,000 new cases of wet AMD are diagnosed each year in the United States • Without treatment, most patients rapidly progress to legal blindness (20/200) in less than 2 years • The impact of visual impairment on direct and indirect costs and on patients’ health-related quality of life is significant 1. National Institutes of Health: National Eye Institute. Vision Problems in the U.S. 2002;20. Available at: http://catalog.nei.nih.gov/productcart/pc/viewPrd.asp?idcategory=43&idproduct=47. Accessed July 31, 2006. 2. Foundation of the American Academy of Ophthalmology. AMD: An Overview of the Disease. Available at: http://www.faao.org/what/AMD/Overview.cfm.Accessed July 31, 2006.
Impact of Visual Impairment on Annual Direct and Indirect Costs • In the United States, annual direct medical costs associated with visual impairment totaled $48.7 billion in 2003.1 • When all indirect costs such as lost productivity are factored in, the total annual cost was $67.6 billion.1 • Loss of vision among elderly women increases the risk of frequent falls.2 • In 2003 more than 1.8 million seniors age 65 years and older were treated in emergency departments for fall-related injuries and more than 421,000 were hospitalized.3 1. NIH National Eye Institute Hu Analysis, available at: http://www.nei.nih.gov/eyedata/hu_estimates.asp#table2. Accessed July 31, 2006. 2. Coleman AL, et al. Ophthalmology. 2004;111:857. 3. CDC.2005. Available at http://www.cdc.gov/ncipc/factsheets/falls.htm. Accessed July 31, 2006.
Patient Reported Visual Function (PRVF) • Importance of PRVF1 • Visual acuity (VA) is the standard visual measurement used in clinical trials. However, VA does not equal visual function or the patient perspective of the impact of vision problems on function • The National Eye Institute Visual Function Questionnaire (NEI VFQ-25) is the measurement tool for self-reported visual function2 • Assesses vision-targeted functioning • Measures impact of vision problems on function for many common eye conditions • Represents the patient perspective of the impact of vision problems on function with attention to • Near activities • Distance activities • Vision-related dependency 1. Presented at ARVO. April 30–May 4, 2006, Fl. 2. Mangione CM, et al. Arch Ophthalmol. 2001;119:1050
What Are Patient-Reported Outcomes (PROs)? • Patient self-reported assessment of the impact of their health status on • Quality of life • Ability to function • PRO data are widely accepted in oncology, medicine, orthopedics, rehabilitation, etc • Use of PROs in ophthalmology reveal the patient’s belief about their level of visual function, which may not be reflective of their visual acuity (VA) • VA is the standard visual measurement used in clinical trials; however, VA does not equal visual function • PROs complement VA data
Visual Acuity Does Not Equal Visual Function These 2 patients have the same VA; however, visual function is markedly different Genentech Data on file. Reprinted with permission.
Visual Acuity Does Not Equal Visual Function Despite normal VA, there is a temporary tilt in vision early after translocation surgery, but this tilt is corrected by the second stage of the eye muscle surgery. Images of grandfather clocks © Copyright 2006, Duke University Eye Center. Reprinted with permission.
NEI VFQ-25Administration and Scoring • Administration • Most patients can complete the questionnaire in 10 minutes • Conducted in-person, by telephone interview, or it can be self-administered • Scoring system (overall and subscales) • Scores range from 0 (worst) to 100 (best) for vision-related functions Mangione CM, et al. Arch Ophthalmol. 2001;119:1050.
NEI VFQ-25 Subscales Mangione CM, et al. Arch Ophthalmol. 2001;119:1050.
NEI VFQ-25 Subscales Mangione CM, et al. Arch Ophthalmol. 2001;119:1050.
How Do We Interpret Changes in the NEI VFQ-25? • SST Report No. 1 1 • A 3-line loss was associated with a 10-point decrease in the NEI VFQ-25 • AREDS Report No. 142 • Changes in NEI VFQ-25 overall and subscale scores of 10 points or more associated with • Clinically significant changes in vision (≥15 letter change) • Progression to advanced AMD from intermediate stage of AMD 1. Miskala PH, et al. Arch Ophthalmol. 2004;122:758. 2. Lindblad AS, Clemons TE. Arch Ophthalmol. 2005;123:1207.
Improvement in Near Activities Placebo (n = 238) Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) 12 10 8 6 4 2 Mean Change in VFQ Score 0 -2 0 1 2 3 4 5 6 7 8 9 10 11 12 -4 -6 -8 Months -10 -12 P values vs placebo: 0.3 mg—.0457 at month 1; .0045 at month 2; <.0001 at months 3, 6, 9, and 12.0.5 mg—.0413 at month 1; .0305 at month 2; <.0001 at months 3, 6, 9, and 12. Presented at ARVO. April 30–May 4, 2006, Fl.
Improvement in Distance Activities Placebo (n = 238) Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) 12 10 8 6 4 2 Mean Change in VFQ Score 0 -2 0 1 2 3 4 5 6 7 8 9 10 11 12 -4 -6 -8 Months -10 -12 P values vs placebo:0.3 mg—.0067 at month 1; <.0001 at months 2, 3, 6, 9, and 12.0.5 mg—>.05 at month 1; .0127 at month 2; <.0001 at months 3, 6, 9, and 12. Presented at ARVO. April 30–May 4, 2006, Fl.
Improvement in Vision-Specific Dependency Placebo (n = 238) Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) 12 10 8 6 4 2 Mean Change in VFQ Score 0 -2 0 1 2 3 4 5 6 7 8 9 10 11 12 -4 -6 -8 -10 -12 Months P values vs placebo: 0.3 mg—>.05 at month 1; .0094 at month 2; .0063 at month 3; .0051 at month 6; .0011 at month 9; .0004 at month 12. 0.5 mg—>.05 at month 1; <.0197 at month 2; .0012 at month 3; <.0001 at months 6, 9, and 12. Presented at ARVO. April 30–May 4, 2006, Fl.
MARINA PRVF Conclusions • Ranibizumab-treated subjects reported improvements in visual function in almost all VFQ subscales at month 12 • Ranibizumab-treated subjects reported clinically meaningful improvements in the VFQ subscales most important in AMD • Near activities • Distance activities • Vision-specific dependency Chang TS, et al. Presented at ARVO. April 30–May 4, 2006, Fl. (Poster 5252/B667)
Key Ocular Serious Adverse Events *1 case reported as uveitis by investigator; †Same subject had 2 episodes each reported as uveitis, received systemic antibiotics once; ‡Same subject had 2 episodes. PDT = photodynamic therapy. Presented at ARVO. April 30–May 4, 2006, FL.
Key Systemic Adverse Events *No serious adverse events of HTN reported during year 1; †Myocardial infarction; ‡Small bowel infarct, chronic asthma/chronic obstructive pulmonary disease (COPD); §Cardiac arrest, COPD; **Cardiac arrest, respiratory arrest, viral syndrome; ††Cardiac failure, chronic heart failure. Presented at ARVO. April 30–May 4, 2006, FL.
VISION Study—Safety • No apparent drug-related SAEs • Few injection-related SAEs (n = 7545 total intravitreal injections) SAEs = serious adverse events. Adapted with permission from Gragoudas ES, et al. N Engl J Med. 2004;351:2805. Copyright © 2004 Massachusetts Medical Society. All rights reserved.
Do We See a Change in Vision-Related QOL in the MARINA Trial?
Secondary Endpoint Mean Change in Visual Acuity Over Time Placebo (n = 238) Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) 10 8 +7.2 +6.5 6 4 17.7 letter difference* 2 0 No. ETDRS Letters 1 2 3 4 5 6 7 8 9 10 11 12 12 -2 17.0 letter difference* -4 -6 -8 -10 -10.5 Month *P < .0001 vs placebo Presented at ARVO. April 30–May 4, 2006, Fl.
Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) Mean Change in VFQ Score from Baseline at Month 12 Placebo (n = 238) Improvement 15 (P < .0001) (P < .0001) (P < .0001) 10 (P < .0001) 5 VFQ score 0 -5 Overall visual function Nearactivities Distance activities Vision-specific dependency -10 -15 Decline Baseline = 0; P-values for combined 0.3 and 0.5 mg ranibizumab vs placebo.Error bars represent the 95% confidence interval of the mean. Chang TS, et al. Presented at ARVO. April 30–May 4, 2006, Fl. (Poster 5252/B667)
Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) Mean Change in VFQ Score from Baseline at Month 12 Placebo (n = 238) Improvement (P < .0001) (P < .0001) 15 (P < .0001) 10 (P < .0001) 5 VFQ 25 Score 0 -5 -10 General vision Vision-specific social function Vision-specific mentalhealth Vision-specificrole difficulties -15 Decline Baseline = 0; P-values for combined 0.3 and 0.5 mg ranibizumab vs placebo.Error bars represent the 95% confidence interval of the mean. Presented at ARVO. April 30–May 4, 2006.
Ranibizumab 0.3 mg (n = 238) Ranibizumab 0.5 mg (n = 240) Mean Change in VFQ Score from Baseline at Month 12 Improvement Placebo (n = 238) 15 10 (P = .260) (P = .125) (P < .0001) 5 (P = .051) VFQ 25 Score 0 -5 -10 -15 Generalhealth Ocularpain Color vision Driving Decline Baseline = 0; P-values for combined 0.3 and 0.5 mg ranibizumab vs placebo.Error bars represent the 95% confidence interval of the mean. Presented at ARVO. April 30–May 4, 2006.
Health EconomicsCost to Society vs Benefits of Treatment • Blindness has a significant impact • Annual medical expenditures • Indirect costs approximately 10 x direct costs • Benefits of treatment • Continuation or resumption of normal daily living activities, including driving • Avoid secondary medical problems, such as broken bones due to falls • Minimal caregiver responsibilities • Decreased likelihood of nursing home admission