AGE-RELATED MACULAR DEGENERATION
380 likes | 2.33k Vues
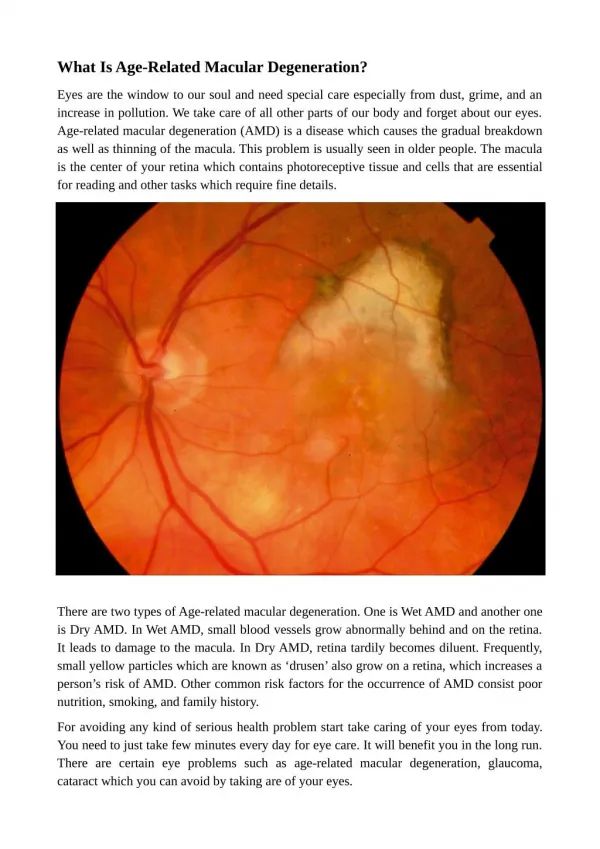
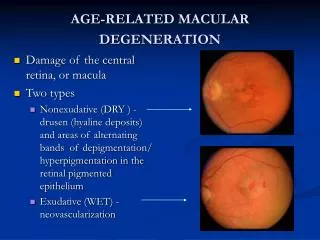
Damage of the central retina, or macula Two types Nonexudative (DRY ) - drusen (hyaline deposits) and areas of alternating bands of depigmentation/ hyperpigmentation in the retinal pigmented epithelium Exudative (WET) - neovascularization. AGE-RELATED MACULAR DEGENERATION. Symptoms

AGE-RELATED MACULAR DEGENERATION
E N D
Presentation Transcript
Damage of the central retina, or macula Two types Nonexudative (DRY ) - drusen (hyaline deposits) and areas of alternating bands of depigmentation/ hyperpigmentation in the retinal pigmented epithelium Exudative (WET) - neovascularization AGE-RELATED MACULAR DEGENERATION
Symptoms Asymptomatic initially Loss of central vision (reduced visual acuity causing difficulties with detail discrimination) Metamorphopsia (i.e., distortion of objects) Central scotomas Increased glare sensitivity Contrast sensitivity Decreased color vision. Peripheral vision remains intact, and the patient does not progress to total blindness AMD Amsler grid
Etiology of AMD • Unclear, but known contributing factors include: • Older age • Smoking • Hypertension • Hyperlipidemia • Vascular insufficiency to the retina and the choroids • History of ultraviolet (UV) light exposure • FHx of AMD (which increases risk three- to fourfold)
Prevention and Treatment • High-dose regimen of vitamin C, vitamin E, beta carotene, and zinc shown to decrease risk of developing vision loss caused by advanced AMD in patients with intermediate AMD or advanced AMD in one eye. • Patients without AMD and those with early AMD did not benefit from supplementation. • Control of vascular disease risk factors, exercise to increase circulation, and sunglasses for UV light protection. • Photodynamic therapy and intravitreal injections of antivascular endothelial growth factor and corticosteroids have shown promise in treating subsets of patients with macular degeneration.
Increased ocular pressure that can damage the ganglion cell layer of the retina Symptoms: loss of peripheral vision that can lead to decreased central acuity, difficulty functioning in dim light, decreased contrast sensitivity, glare disability, and decreased dark/light adaptation. Risk factors: Age > 40, Hispanic, African American, Family history, diabetes, HTN, eye injury, myopia, chronic steroids Treatment: topical prostaglandins, beta blockers, adrenergics, carbonic anhydrase inhibitors, and oral medications, laser therapy, and filtering surgery. GLAUCOMA
Opacifications of the crystalline lens of the eye Risk factors: Age, female sex, corticosteroid use, diabetes, smoking, ocular UV-B light exposure Symptoms: decreased visual acuity, decreased color perception, decreased contrast sensitivity, and glare disability Treatment: alter prescriptions for eyeglasses or contacts, tobacco cessation, UV protection, surgical extraction. CATARACTS
Nonproliferative - dilated retinal veins, intraretinal hemorrhages, microaneurysms, cotton wool spots, hard exudates, and macular edema Proliferative - neovascularization, vascular fibrosis, and preretinal and vitreous hemorrhages DIABETIC RETINOPATHY
Symptoms: decreased visual acuity, contrast sensitivity, color perception, and dark/light adaptation, glare disability, distortion, and scotomas Treatment: Photocoagulation DIABETIC RETINOPATHY
Screening • ADA recommends that children with diabetes have an initial eye examination after 10 years of age if they have had diabetes for three to five years, followed by annual examinations thereafter • AAO recommended eye exam schedule • Normal examination or minimal nonproliferative retinopathy– annually • Mild to moderate nonproliferative retinopathy without macular edema - every 6 to 12 months • Severe nonproliferative diabetic retinopathy – every 2 to 4 months
Quiz • Which one of the following is an adverse effect of alpha blockers? A. Increased incidence of prostate cancer. B. Increased incidence of high-grade prostate cancer. C. Orthostatic hypotension. D. Ejaculatory dysfunction.
Which one of the following statements about the surgical treatment of benign prostatic hypertrophy is correct? A. Laser prostatectomy is associated with decreased libido. B. Transurethral incision of the prostate is more likely to cause retrograde ejaculation than transurethral resection of the prostate (TURP). C. Transurethral needle ablation is recommended only for men with severe symptoms who are not surgical candidates. D. Retreatment rates are higher with transurethral microwave therapy than with TURP.
Which one of the following medications is recommended for the treatment of tinea capitis in children? A. Oral terbinafine (Lamisil). B. Oral ketoconazole (Nizoral). C. Topical ketoconazole. D. Oral itraconazole (Sporanox).
Which one of the following is the recommended initial test for the diagnosis of tinea unguium (onychomycosis)? A. Histologic analysis. B. Potassium hydroxide microscopy. C. Fungal culture. D. Wood's lamp examination.
Which one of the following statements about seizures in patients with primary brain tumors is correct? A. Patients who present with seizure have a worse prognosis than those who do not present with seizure. B. Patients who present with seizure have a better prognosis than those who do not present with seizure. C. Seizures are more common in patients with high-grade gliomas. D. Long-term seizure prophylaxis is recommended for all patients after surgery.
Which one of the following imaging studies is preferred for the initial anatomic evaluation of brain tumors? A. Functional magnetic resonance imaging (MRI). B. Computed tomography. C. Gadolinium-enhanced cranial MRI. D. Positron emission tomography.
A patient has dilated retinal veins, intraretinal hemorrhages, microaneurysms, cotton wool spots, and hard exudates. There is no macular edema. Which one of the following diagnoses is the most likely? A. Age-related macular degeneration. B. Nonspecific changes of aging. C. Diabetic retinopathy. D. Cataracts. E. Open-angle glaucoma.
Which one of the following treatments represents optimal management of diabetic retinopathy without macular edema? A. Intraocular vitamins. B. Tight control of blood glucose. C. Laser photocoagulation. D. Oral corticosteroids.
X-Type • The initial evaluation of patients with symptoms of benign prostatic hyperplasia typically includes which of the following? A. Digital rectal examination. B. Urinalysis. C. Prostate-specific antigen measurement. D. Serum creatinine measurement.
Which of the following statements about the management of tinea corporis is/are correct? A. Culture confirmation of the diagnosis is recommended. B. Diagnosis is usually clinical or based on potassium hydroxide microscopy findings. C. Most patients require oral therapy. D. Topical antifungals are usually sufficient for treatment.
Which of the following signs and symptoms is/are seen at presentation in one third or more of patients with primary brain tumors? A. Nausea or vomiting. B. Headache. C. Papilledema. D. Memory loss.
A 54-year-old patient with 20/70 vision has had a recent worsening of a physiologic tremor. Which of the following statements is/are correct? A. He is legally blind. B. A stand magnifier is an appropriate low-vision aid for this patient. C. He should be examined by an ophthalmologist or optometrist every two to four months. D. He is at risk for falls.
References • EDWARDS J. Diagnosis and Management of Benign Prostatic Hyperplasia. American Family Physician. May 15, 2008 • ANDREWS M, BURNS M. Common Tinea Infections in Children. American Family Physician. May 15, 2008 • CHANDANA S, MOVVA S, ARORA M. Primary Brain Tumors in Adults. American Family Physician. May 15, 2008 • ROSENBERG E, SPERAZZA L. The Visually Impaired Patient. American Family Physician. May 15, 2008