ACNE
ACNE. Dr. Sandeep Rondla South Birmingham VTS. Introduction. Acne is a disease of pilosebaceous follicles present on the face and the upper trunk and are under androgenic control. Affects most of the adolescent population, in 20% of these it is clinically significant

ACNE
E N D
Presentation Transcript
ACNE • Dr. Sandeep Rondla • South Birmingham VTS
Introduction • Acne is a disease of pilosebaceous follicles present on the face and the upper trunk and are under androgenic control. • Affects most of the adolescent population, in 20% of these it is clinically significant • Both sexes involved, peak at 16 - 20 years • In chronic disease, it persists till the mid 20s, in 7% until 40-50 yrs. • Rare in infancy
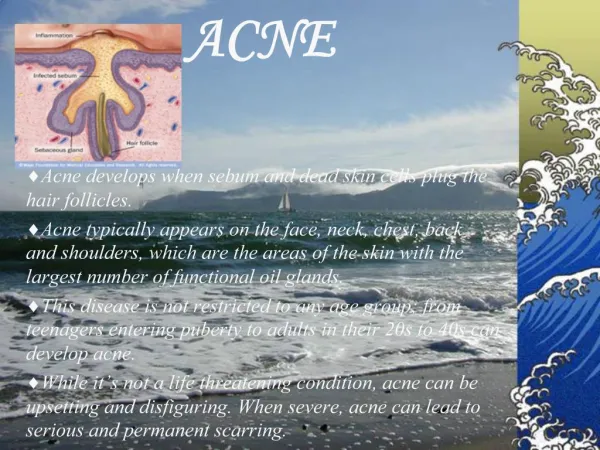
Aetiology • 3 types of follicles in the skin : hair (beard), vellus and sebaceous • Acne involves sebaceous follicles - seen on face, back and chest. • Factors in acne formation • increased sebum production • ductal hyperprolifertaion (comedone formation) • colonisation of the duct with Propionibacterium acnes • inflammation • inflamation
Increased sebum production • Patients with acne produce more sebum than controls • No evidence of significant hormonal abnormalities, hence do not need investigation • Evidence suggests that acne is an end-organ hyper-response of sebaceous glands to circulating hormones • Androgens of adrenal and gonadal origin stimulate sebum production
comedone formation whitehead Vs blackhead • Comedone formation is the result of ductal corneocytes accumulating in the ductal lumen. • Comedone present clinically as blackheads and whiteheads • A whitehead is referred as a closed comedone as it very small orifice with many proinflammatory substances in the duct contents. • A black head is referred to as a open comedone with large orifice. • Whiteheads are more prone to develop into inflammatory lesions than blackheads. • Treatment should be aimed at reducing microcomedones which usually precede these lesions.Topical retinoids are the treatment of choice.
P.acnes • Normal commensal of the skin, esp in sebum rich areas • Infection occurs when there is colonisation of the pilosebaceous duct with p. acne, usually early after comedone formation • Exact mechanism of colonisation is not known • Evidence suggests : role of micro-environment in acne prone glands
inflammation • Inflammation is type IV cell mediated immune reaction • Specific antigen not identified • In pustule stage : polymorphonuclear leucocytes • In intense papular stage : giant cell response with associated duct rupture • Inflammation leads to scarring due to loss of or increase collagen
clinical features • Seborrhoea - greasiness • Comedones • Superficial inflamed lesions - papules, pustules, macules • Deep inflamed lesions - nodules and deep pustules • Scars • Post inflammatory pigmentation
acne grading • MILD - Predominantly consists of non-inflammatory comedones • MODERATE - Mixture of non-inflammatory comedones and inflammatory papules and pustules • SEVERE - Presence of nodules and cysts along with preponderance of inflammatory papules and pustules
differential diagnosis • Perioral dermatitis • Seborrhoeic eczema • Rosacea • Pomade acne • Steroid induced acne Pomade acne
investigations • Rarely needed • Hormonal investigations to be done if hirsuitism or very irregular menses (PCOD) • Erythromycin resistant P. acne seen in 65% and tetracycline resistance seen in 20% - culture might be useful • Patients on minocycline should have blood tests 6 monthly to check LFTs, ANF and pANCA • If starting on oral isoretinoin - liver enzymes and lipids at baseline / 1 month after starting treatment and every 3 months there after • Pregnancy test - pre therapy and 5 weeks post therapy. Monthly pregnancy test recommended.
treatment principles • Discussion with patient • Choice of Topical therapy • Choice of Oral therapy • Choice of Physical therapy • Combined therapy
discussion with the patient • Time spent by the general practioner in discussing acne with the patient should emphasise the following : • Acne is a chronic disease. • A treatment strategy is needed and it is likely that long therapy will be required. • Acne is a slow responding disorder with little improvement in the first 3-5 weeks. • There is a need for continued compliance • There is no evidence that fatty foods or chocolate adversely affect acne. • Certain physiological events may influence acne,for example :stress may make acne worse • Premenstrual flare is common in 70% of females. Sunshine often helps acne but often temporarily.
topical therapy • Mild disease • Combination with oral antibiotics in moderate disease • Combination with hormonal therapy in females • Maintenance therapy after oral therapy has been discontinued
DIANETTE • Dianette has a product license for severe acne but is not licensed as an oral contraceptive in the UK. • It achieves improvement in 75 - 90 % of female patients. • Relative risk of VTE is slightly higher compared to other COC pills • Should be withdrawn 3 to 4 cycles after the acne is clear • Once Acne is clear - low androgenic effect pill like Marvelon , Cilest or Yasmin prescribed for contraception rrequired
treatment failure • Wrong Diagnosis • Compliance Problems - common problem. Must be stressed to patient • P.acnes Resistance - increasing problem. Commonly seen with Erythromycin & Clindamycin
referral guidelines to secondary care - NICE • Patients who have severe physical disease. • Patients who have moderate disease but have failed to respond to 6 months of adequate oral and topical therapy. • Patients in whom there are significant psycho-social problems from acne. • Patients with significant problems with scarring / who may be at risk of scarring. • Patients suspected of significant hormonal disease.
treatment algorithm Acne grade Choice of treatment Maintenance therapy Mild acne (Comedones +/- inflammatory lesions Topical retinoids +/- Benzoyl peroxide / Topical antibiotics Success Failure Combination therapy Oral Antibiotic + Topical retinoid +/- Benzoyl peroxide Success Moderate acne (mild to moderate papular / pustular) Topical retinoids +/- Benzoyl peroxide Failure Systemic isoretinoin +/- Hormonal therapy (females) Success Severe acne (severe nodulocystic)
Thank You • Questions