Acne
Acne. Prepared by : Yazan Mohammad Khdour Hanady Adnan Khdour. Overview. Definition: Acne vulgaris is disorder of piloseceous units. Location: Mainly is the face, chest and back. It is the most common skin disease of adolescence; it affects about 85% of all people between 12 & 24.

Acne
E N D
Presentation Transcript
Acne Prepared by : Yazan Mohammad Khdour Hanady Adnan Khdour
Overview Definition: Acne vulgaris is disorder of piloseceous units. Location: Mainly is the face, chest and back. It is the most common skin disease of adolescence; it affects about 85% of all people between 12 & 24
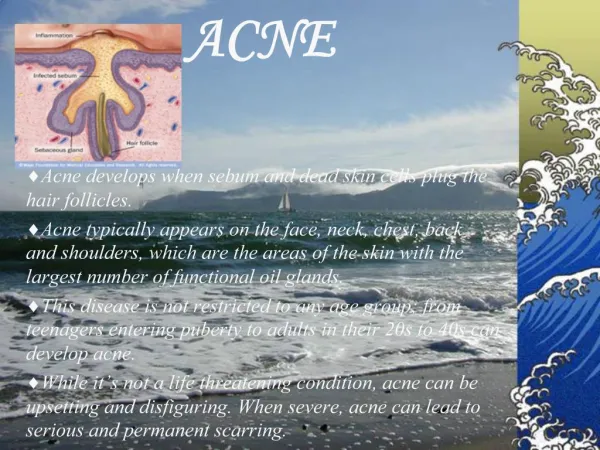
Origins and pathophysiology The pathogenesis of acne vulgaris involves three events: 1.Increased sebum production 2.Abnormal clumping of epithelial horny cells within the pilosebaceous unit. 3.Presence of propionibacterium acnes (G+ anaerobe).
Increased sebum production Sebum production is regulated by androgens which are secreted in both sexes beginning at puberty One of these androgens , testosterone is converted to DHT DHT level induce the sebaceous glands to increase in size and activity, resulting in increased amount of sebum
Abnormal clumping of epithelial horny cell within the pilosebaceous unit: Normally, keratinized horny cells are sloughed from the epithelial lining of the pilosebaceous duct in hair follicles and are carried to the skin surface with a flow of sebum In the patient with acne , the keratinization process is abnormal, characterized by increasing adherence and production of follicular epithelial cells. This process is called retention hyperkeratosis, and it results in obstruction of the outflow of the pilosebaceous unit.
Presence of propionibactrium acnes (G+ anaerobe) People with acne have higher counts of p.acnes than without acne. P.Acnes produces several enzymes , including lipases that break down sebum TAG to short chain free fatty acid (FFAs), which is irritating , cause comedones and inflammation.
Sequence of acne legion development: A. Mechanical blockage of apilosebaceous duct by clumped horny cells results in closed comeddo (i.e., white head)
B. When a closed come do develops, it can form either: 1.Papule 2.Or an open come do (i.e., blackhead) The dark color of the blackhead is attributed to a combination of melanin; oxidized lipid, And keratinocytes, not to dirt.
C. The lesion may enlarged and fill with pus which is termed a pustule. D. In more sever cases of acne, papules may develop in to nodules or cysts.
Classification: It is important to differentiate noninflammatory from inflammatory acne to determine the best treatment approach.
Complicating factors Drug & Hormones Many topical and systemic medications may: 1.Make acne worse 2.Induce acne _ like eruptions ( acneiform lesion). (e.g., Br, I, topical coal tar products, androgens, phenytoin, progestins, lithium, and corticosteroids). Stress, chocolate, sugar, nuts : dose not cause acne but may exacerbate
Diet : there is little evidence to support a relationship between diet and acne. The majority of dermatologists today make the following recommendation regarding diet: I.The patient should be eating a well-balanced diet, excess fats and simple carbohydrates should be avoided. II.The patient who insists that certain foods cause exacerbation of acne should be avoided.
Physical trauma or irritation can promote the rupture of plugging follicles which can produce more inflammatory reaction Cosmetics: some cosmetics bases and certain cosmetic ingredients are comdogenic ( block follicles) Menstrual cycle: fluctuation in the level of progesterone are the probable cause.
Environmental factors: Very humid environment or heavy sweating lead to keratin hydration , swelling and decrease in the size of pilosebaceous follicle , which results in duct obstruction.
Treatment and care 1.Most patient can be treated successfully with either topically or systemically medication. 2.Most effective treatment programs may take several weeks to produce any clinical improvement. 3.People affected with acne should avoid any thing worsen the condition(i.e., cosmetics, clothing, cradling the chin with the hand),
4.The number and type of lesions should be determined to assess the therapeutic responses. 5.Self-treatment with OTC agents is appropriate only for patients with noninflammatory grade I of mild to moderate severity.
Cleansing and recommendations People with oily skin should make gentle cleansing 2-3 times daily with facial soaps (Dove, Neutrogena) Medication soaps containing sulfur, resorcinol, or salicylic acid are of little value because the medication rinses away. Patients with mild acne benefit from cleansers containing pumice, polyethylene
Approaches to treatment 1.Unblocking the sebaceous duct 2.Decreasing the amount of sebum that is recreated 3.Changing the composition of sebum to make it less irritating by decreasing the population of P.acnes.
Nonprescription topical medications: A.Benzoyl peroxide (2.5%-10%) For example: Clearasil Maximum Strength Acne treatment cream, PanOxyl aqua Gel. Effect: Irritant, drying, peeling, comedolytic, and antibacterial effects. 1.A beneficial effect should be noticed within 2 weeks 2.Adverse effect: burning or stinging sensation, contact dermatitis.
MOA: Benzoyl peroxide has dual action ,so it is effective against both inflammatory and non inflammatory acne: i.Decomposes to release O2 which kills P.acnes. ii.As an irritant: it increases turn over rate of epithelial cells.
B.Salicylic acid (0.5%-2%), an irritant keratolytic agent, so increased turnover of epithelial lining. C.Sulfur (3%-8%) combined with resorcinol(2%), or monoacetate (3%) Example: Clearasil adult care acne treatment cream 1.Sulfur is a keratolytic agent and has antibacterial actions. 2.Sulfur traditionally has been recognized as less desirable product because it: May be acnegenic and it has an offensive color and odor.
AZELAIC ACID Reduce p.acne resistance Natural product
Prescription medication Topical prescription agents 1.Tretinoin: ( Vit A acid, Trans retinoic acid, retin A) increases the turn over of non adhering horny cell in the follicular canal which results in come do clearing and inhibits new come do development. Effectiveness : most effective topical agent against acne especially comedones. Best use for non-inflammatory acne, may be used with antibiotics or benzoyl peroxide for inflammatory acne.
Side effects: Excessive irritation, erythema, peeling, Sever sun burn. Applications: Cream is less irritating than gel, but gel is good for oily skin The retinoids should be applied 30 min after washing because moisture on the skin increases absorption and irritating. To prevent irritation a product should be applied every other day for 2 weeks.
2.Adapalene(differin), retinoid like compound Effectiveness :equivalent to tretinoin with less irritation. Used as alternative to retinoin. Applied in the morning because it has less photosensitivity.
3.Tazarotene gel & cream( Tazorac): Is a retinoin prodrug for mild to moderately sever facial acne. It has similar efficacy and precautions as treinoine Side effects: It is dose-related, include itching, coma, burning, stinging, erythema.
4.Topical antibiotics: I.Erythromycine(eryderm) II.Tetracycline III.Clindamycin(cleocin-T)
Topical antibiotics are more effective in combination with topical benzoyl peroxide and retinoids to protect against bacterial resistance. Benzoyl peroxide + erythromycin = Benzamycine Benzoyl peroxide + Clindamycin = BenzaClin
MOA: Suppression of P.acnes and minimize inflammation Application: Directly to acne site, thus minimizing serious side effects from oral administration Side Effects: Mild burning, irritation, Tetracycline may cause yellow staining of the skin.
Systemic prescription agents Oral antibiotic/ Anti infective: Tetracycline: Most frequently used, preferred because its effectiveness, low cost. Erythromycin(E-Mycin): Use as alternative to tetracycline. Monocycline(Minocin) or Doxacycline (Vibramycin) Trimethoprim-sulfamethoxazole (bactrim,Septra)
Oral Isotretinoin (Accutane)vit A derivative indicated for sever nodulocytics acne MOA: It reduces sebum production and keratinizeation and P.acnes. Side Effects: 1.Mucocutaneous dryness 2. Serum level of: TAG , Cholesterol, liver enzymes
3.Teratogenic ( not given to pregnant) 4.Psychiatric effects: depression.
Anti androgens and hormones. Estrogen: sebum production Some progestin agents in oral contraceptives (norethindrone) stimulate sebum secretions that results in acne.
Some OTC products available in Palestinian pharmacies : Clearx (5%, 10% Benzoyl Peroxide) PanOxyl (Benzoyl Peroxide gel) Acne Free (Herbal)