Download
1 / 38
380 likes | 905 Vues
Salivary Glands: Major. Salivary Glands: Parotid. Salivary Glands: Submandibular. Salivary Glands: Sublingual. Salivary Glands: Minor. Salivary Glands: Minor. Developmental Anomalies of Salivary Glands. Heterotopic SG tissue, Stafne's idiopathic bone cavity.. Acute Bacterial Sialadenitis. Clinical features:Rapid onset.Swelling of involved gland.Pain, fever, malaise.Redness of overlying skin.Pus may be expressed from duct..

E N D
1. Dent 356-10 Laboratory Session 4 Diseases of Salivary Glands Dr. Huda Hammad
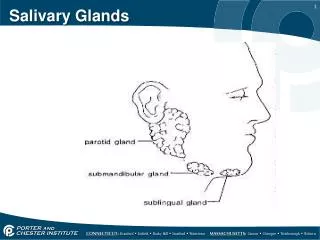
2. Salivary Glands: Major
3. Salivary Glands: Parotid
4. Salivary Glands: Submandibular
5. Salivary Glands: Sublingual
6. Salivary Glands: Minor
7. Salivary Glands: Minor
8. Developmental Anomalies of Salivary Glands Heterotopic SG tissue, Stafne�s idiopathic bone cavity.
9. Acute Bacterial Sialadenitis Clinical features:
Rapid onset.
Swelling of involved gland.
Pain, fever, malaise.
Redness of overlying skin.
Pus may be expressed from duct.
10. Chronic Bacterial Sialadenitis Progressive chronic inflammation of submandibular gland may result in almost complete replacement of parenchyma by fibrous tissue, which may be mistaken for a tumor (chronic sclerosing sialadenitis).
11. Chronic Bacterial Sialadenitis Histopathology:
- varying degrees of ductal dilatation.
- hyperplastic ductal epithelium.
- periductal fibrosis.
- acinar atrophy & replacement by fibrous tissue.
- chronic inflammatory infiltration.
12. Mumps (Epidemic Parotitis)
13. Salivary Calculi (Sialoliths)
May form in ducts within the gland.
Or in main excretory duct.
14. Salivary Calculi (Sialoliths) Calculi may be detected by palpation and on radiographs.
15. Salivary Calculi (Sialoliths) Thought to form by gradual deposition of calcium salts around an initial organic nidus which may consist of altered salivary mucins with desquamated cells and microorganisms.
16. Necrotizing Sialometaplasia Presents a s a deep, crater-like ulcer which may mimic a malignant ulcer.
Ulcer may be preceded by an indurated swelling.
17. Necrotizing Sialometaplasia Histopathology:
Lobular necrosis (coagulative), squamous metaplasia of ducts & acini, mucous extravasation, inflammation.
Surrounding palatal mucosa shows pseudoepitheliomatous hyperplasia.
- Feature may be mistaken for SCC or mucoepidermoid carcinoma.
18. Sj�gren Syndrome: Clinical Features Xerostomia Rapidly progressive caries
19. Sj�gren Syndrome: Clinical Features Keratoconjuctivitis sicca manifests as:
dryness of eyes
conjunctivitis
gritty, burning sensation.
20. Sj�gren Syndrome: Clinical Features Salivary gland enlargement is variable.
21. Sj�gren Syndrome: Histopathological Features Lymphocytic infiltration, initially around intralobular ducts, eventually replacing the whole affected lobules.
Acinar atrophy.
Proliferation of duct epithelium to form epimyoepithelial islands.
The appearance is described as myoepithelial sialadenitis, the same as benign lymphoepithelial lesion.
Unlike lymphoma, the infiltrate does not cross interlobular CT septa.
22. Sj�gren Syndrome: Histopathological Features Minor salivary glands show focal collections of lymphoid cells related to blood vessels adjacent to ducts.
The number of foci reflects the severity of the disease.
There may be acinar atrophy.
23. Sj�gren Syndrome: Sialography
�Snowstorm� pattern, �cherry tree in blossom� appearance.
24. Sj�gren Syndrome Approximate frequencies of serological abnormalities & autoantibodies in primary & secondary Sj�gren Syndrome
25. HIV-Associated Salivary Gland Disease Parotid enlargement may be due to:
Persistent glandualr lymphadenopathy.
Multiple lymphoepithelial cysts.
26. Pleomorphic Adenoma (Mixed Tumor) Slowly growing, painless, rubbery swelling with intact overlying skin or mucosa.
27. Pleomorphic Adenoma: Histopathologic Features
Composed of cells of epithelial and myoepithelial origin.
Great variety with complex intermingling of components & mesenchyme-like areas, hence the 2 names.
28. Pleomorphic Adenoma: Histopathologic Features Although benign, CT capsule is not always complete.
Clearly demarcated , but apparently isolated nodules may be seen within or even outside the capsule give the impression of invasive growth.
Serial sections show that these represent outgrowths of the main mass.
These islands explain the need for excision with a margin to avoid recurrence.
29. Pleomorphic Adenoma: Histopathologic Features Considerable variation in arrangement of epithelial and stromal components between different tumors and within different areas of same tumor.
Intercellular material varies in quantity and quality: fibrous, hyalinized, myxoid, chondroid, or myxochondroid.
Malignant transformation can occur, usually in tumors present for many years.
30. Pleomorphic Adenoma: Histopathologic Features Pelomorphic adenoma of the parotid gland. A well-defined tumor has a thin fibrous capsule. Normal serous glands are also seen (N).
31. Pleomorphic Adenoma: Histopathologic Features Tumor cells arranged in tubules (arrow) and cell cords (arrowhead). The background is myxoid.
32. Pleomorphic Adenoma: Histopathologic Features Tubular structures in pleomorphic adenoma. The tubules are composed of two layers of cells.
The inner layer is made up of ductal epithelial cells with eosinophilic cytoplasm (arrowhead).
The outer layer is composed of myoepithelial cells with scanty cytoplasm (arrow).
The background is myxoid (Note the clear spaces between epithelial cells)
33. Pleomorphic Adenoma: Histopathologic Features Cell cord structures in pleomorphic adenoma. The cell cordsare composed of myoepithelial cells with spindle nuclei (arrow)
34. Pleomorphic Adenoma: Histopathologic Features Epithelial-duct cells and myoepithelial-type cells.
Polygonal, spindle, stellate, or plasmacytoid cells thought to be derived from myoeoithelium.
35. Pleomorphic Adenoma: Histopathologic Features Areas of squamous metaplasia and keratin pearl formation may be present.
36. Pleomorphic Adenoma: Histopathologic Features Chondroid stroma in pleomorphic adenoma (arrow). The stroma resembles the hyaline cartilage.
37. Pleomorphic Adenoma: Histopathologic Features Chondroid stroma in pleomorphic adenoma. The stroma resembles hyaline cartilage.
38. Warthin Tumor (Papillary Cystadenoma Lymphomatosum) Multiple, irregular cystic spaces ( C ) of variable size containing mucoid material.
The lining of the cysts have small projections that represent the papillary structures.
39. Warthin Tumor (Papillary Cystadenoma Lymphomatosum) Histopathologic Features:
Multiple, irregular cystic spaces containing mucoid material.
Separated by papillary projections of tumor tissue.
Consists of:
Epithelial component: double-layered epithelium lining cystic spaces in papillary arrangement.
Lymphoid component: within stroma.
40. Basal Cell Adenoma Consists of cytologically uniform basaloid cells arranged in a variety of patterns.
Well-encapsulated.
41. Canalicular Adenoma Consists of anastomosing strands of epithelial cells arranged in canalicular structures.
May be partly or grossly cystic due to degeneration of loose vascular stroma.
42. Mucoepidermoid Carcinoma Most arise in parotid.
Often presents clinically in a similar to pleomprphic adenoma.
Grossly cystic tumors may be fluctuant.
More aggressive tumors may cause pain and ulceration.
43. Mucoepidermoid Carcinoma: Histopathologic Features Characterized by presence of 3 cell types: squamous (epidermoid), mucous, and intermediate.
Relative proportions and arrangements of cell types are used to distinguish between:
High grade MEC.
Low grade MEC.
44. Mucoepidermoid Carcinoma: Histopathologic Features Low grade MEC:
Well-differentiated.
Mucous and epidermoid cells predominate.
>50% mucous cells.
No cellular pleomorphism.
Often cystic, cysts being lined by mucus-secreting cells.
Epidermoid cells present in strands or clumps, may show keratinization.
Rupture of mucin-containing cysts may lead to inflammation.
Advance on a broad, pushing front.
45. Mucoepidermoid Carcinoma: Histopathologic Features Low power view of one area lining the lumen. Since most of this lesion is cystic and there is orderly production of mucin, this component would be classified as a low grade mucoepidermoid carcinoma.
46. Mucoepidermoid Carcinoma: Histopathologic Features High grade MEC:
Poorly differentiated.
Epidermoid and intermediate cells predominate.
< 10% mucous cells.
Nuclear & cellular pleomprphism and atypia.
Cystic spaces not prominent.
Ill-defined and highly infiltrative.
47. Mucoepidermoid Carcinoma: Histopathologic Features High grade MEC:
Diffrentaition from SCC may be difficult.
Special stains are used sometimes to demonstrate intracellular mucin, e.g. PAS, mucicarmine.
48. Acinic Cell Carcinoma: Histopathologic Features Microscopically non-encapsulated, may show invasive pattern.
The most common variants consist of sheets or acinar groupings of large, polyhedral cells with basophilic, granular cytoplasm, similar to serous acinar cells.
49. Adenoid Cystic Carcinoma May present as slowly enlarging tumors like pleomorphic adenoma, but pain and ulceration are much more common.
50. Adenoid Cystic Carcinoma: Histopathologic Features Wide spectrum of appearances.
Most commonly, epithelium arranged as ovoid & irregularly shaped islands or anastomosing cords and strands in scanty Ct stroma.
Numerous microscopic cyst-like spaces within epithelial islands produce a cribriform or �Swiss cheese� pattern.
Epithelium consists of small, uniform, basophilic cells.
Rare mitoses.
51. Adenoid Cystic Carcinoma: Histopathologic Features Perineural invasion.
52. Carcinoma Arising in Pleomorphic Adenoma Histological diagnosis requires evidence of pre-existing pleomorphic adenoma.