Download
1 / 1
10 likes | 114 Vues
Explore factors affecting nafcillin clearance, identify associations with plasma concentrations and adverse events, and assess dosing implications in a diverse patient sample.

E N D
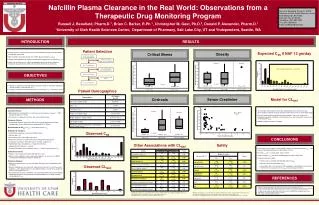
Abstract #A-477 Nafcillin Plasma Clearance in the Real World: Observations from a Therapeutic Drug Monitoring Program Russell J. Benefield, Pharm.D.1, Brian C. Barker, R.Ph.1, Christopher M. Gast, Ph.D.2, Donald P. Alexander, Pharm.D.1 1University of Utah Health Sciences Center, Department of Pharmacy, Salt Lake City, UT and 2Independent, Seattle, WA Russell J. Benefield, Pharm.D., BCPS University of Utah Health Sciences Center 50 N Medical Dr, Rm A-050 Salt Lake City, UT 84132 Telephone: (801) 587-0587 Fax: (801) 585-0403 Email: u0789327@utah.edu RESULTS INTRODUCTION • Despite 50 years of clinical experience, the pharmacokinetic profile of nafcillin (NAF) is incompletely understood. • Many conditions could conceivably alter nafcillin plasma clearance (CLNAF) • Product labeling provides no guidance for NAF dosing adjustments for altered CLNAF [1] • Unlike most medical centers, a NAF microbiological assay has been available for therapeutic drug monitoring (TDM) at the University of Utah for over 20 years. Patient Selection Obesity Critical Illness Expected CSS if NAF 12 gm/day Previous Current Proposed Supratherapeutic CSS > 40 mg/L OBJECTIVES 93 NAF concentrations from 62 Adult Inpatients • Review our experience with NAF TDM in a diverse sample of “real-world” patients to identify variables associated with CLNAF. • Examine associations between NAF plasma concentrations (Css) and adverse events P = 0.97 P = 0.01 CLNAF = 32.0 Median = 14.1 Median = 13.6 Median = 9.1 Median = 17.4 2 NAF concentrations Drawn Before Steady State Patient Demographics 91 CSS from 62 Patients Serum Creatinine Cirrhosis METHODS Model for CLNAF 22 CSS Influenced by Concomitant Antibiotics 69 CSS from 46 Patients • An interaction effect between bacteremia, hyperbilirubinemia, and cirrhosis was observed which required exclusion of patients with cirrhosis from our multivariate model • Our early model identified hyperbilirubinemia, diabetes, and serum creatinine as independent variables negatively associated with CLNAF and male gender as positively associated with CLNAF • Additional model refinement is ongoing • Inclusion Criteria: • Adult inpatients receiving NAF as a continuous infusion between January 1st, 2007 through December 31st, 2012 • At least one CSS obtained (>12 hours after start of NAF infusion) • Exclusion Criteria: • Concomitant antibiotics with activity against the indicator organism of the NAF microbiological assay (Staphylococcus epidermidis ATCC 12288) • Determination of CLNAF: CLNAF = rate of NAF infusion / CSS • Definition of Variables: • Critical illness: presence in ICU plus ≥2 SIRS criteria • Obesity: BMI > 30 • Severe burn injury: >30% body surface area • Bacteremia: infection associated with at least one positive blood culture • Congestive heart failure: New York Heart Association stage III or IV • Hyperbilirubinemia: Total bilirubin > 2 mg/dL for ≥ 48 hours • Hypoalbuminemia: Albumin < 3 gm/dL • Concomitant hepatic efflux transporter inducer: > 14 days treatment prior to CSS • Safety Assessment: • Progress notes reviewed for known NAF adverse events • Adverse events defined as new or worsening symptoms, or an increase in DMID severity grade following the initiation of nafcillin [2] • Statistical Analysis: • Bivariate associations were assessed by Mann-Whitney U test or Spearman’s rank correlation • Bivariate comparisons were made with subject-level means for CSS and CLNAF when multiple CSS were obtained from the same patient without a change in the variable of interest (e.g. vasopressor use) • A generalized least squares model was constructed by stepwise AIC-based selection followed by backward selection based on individual Wald tests to identify variables associated with CLNAF 2 CSS from Spurious Lab Draws Current Previous 67 CSS from 45 Patients Observed CSS P = 0.045 Median = 6.3 Median = 16.0 Median = 14.1 CONCLUSIONS Safety Other Associations with CLNAF • In this largest series to date, several variables appear to be associated with CLNAF. This may have practical implications for NAF dosing schemes • Elevated CSS were associated with adverse effects • A wide range of CLNAF was observed highlighting the utility of NAF TDM • Contrary to previous reports: • Cirrhosis was associated with markedly reduced CLNAF • Obesity was not associated with CLNAF • Associations with serum creatinine and hemodialysis may indicate renal clearance mechanisms have a greater role in CLNAF than previously described Observed CLNAF REFERENCES Nafcillin for injection [package insert]. Princeton, NJ: Sandoz Pharmaceuticals Corp; 2012 Division of Microbiology and Infectious Diseases, National Institute of Allergy and Infectious Diseases, National Institutes of Health. Microbiology and Infectious Diseases clinical research policies, guidance, and tools. Available at http://www.niaid.nih.gov/LabsAndResources/resources/DMIDClinRsrch/pages/toxtables.aspx. Marshall JP, et al. Gastroenterology 1977;73:1388-92. Yuk J, et al. J Infect Dis 1988;157:1088-9. aMultiple intra-subject CLNAF observations were counted separately if there was a change in variable status (e.g. hyperbilirubinemia). Consequently, total n for each variable may be >45 bNo patients with severe burn injuries were included in this cohort aMultiple intra-subject CSS observations were counted separately if there was a change in adverse effect status (e.g. before and after diarrhea resolved). Consequently, total n for each adverse effect may be >45 bNo seizures or anaphylactic events were observed. There was one case of interstitial nephritis (CSS > 60 mg/L)





















