Download
1 / 23
240 likes | 391 Vues
Understand the physiology of skeletal muscles, from anatomy to contraction mechanisms, and the impact of aging on muscle tissue. Learn about sarcopenia and myoplasticity effects, and the importance of exercise training for muscle health.

E N D
Aging of Skeletal Muscle Dr. Franco Navazio
Muscles There are 660 skeletal muscles in adult humans These constitute 45% to 50% of the normal body weight Their primary purpose is to provide “MOTILITY” In addition, they represent the major site for: - energy transduction - energy storage - primary support system
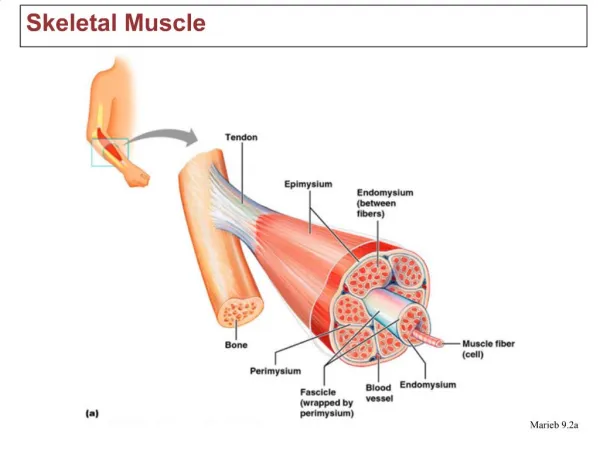
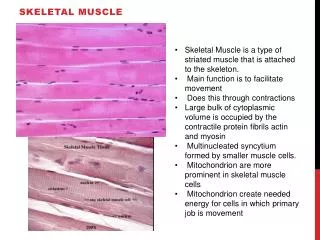
Anatomy Skeletal muscle is composed of Muscle fascicles are composed of Muscle fibers (multinucleated cells, the longest in the body) Each fiber is composed of MYOFIBRILS and, within the myofibril structure, the contracting machinery is the SARCOMERE Sarcomeres are composed of digital thin filaments, the “ACTINS,” and interdigitated thick filaments: the MYOSINS
Anatomy • 2 membranes surround the muscles: • outer membrane: the basement membrane (very permeable to solutes and proteins or to other metabolites) • inner membrane: SARCOLEMMA is located just beneath the plasma membrane (a true cell boundary) • An intact sarcolemma is critically important: • it maintains a proper acid-base balance of the fibers • propagates the action potential (starting at the neuromuscular plaque leading to the muscle contraction)
Contraction The actors: • Ca++ passes through the sarcolemma; in its presence there is hydrolysis of ATP (ADP+P) which releases energy • ADP binds to ACTIN: meanwhile, a regulatory protein (enzyme) TROPONIN (activated by this energy) binds to MYOSIN forming TROPOMYOSIN--shifting the ACTIN helix and leading to CONTRACTION End result: the ACTOMYOSIN complex • Contraction could involve lengthening or shortening mechanisms, depending on the movement pattern • MEMO the TETANIC contraction
GENDER EFFECTIn both sexes, strength & power can only be obtained after myelination of the afferent nerves, reached at maturity. Maximum gain in muscle strength is reached in boys by testosterone & in girls by estrogens, all of these stimulated by gonadotropins. Low levels of testosterone and other androgens (e.g. androstenedione) are also present in girls. The higher fat percentage induced in girls by estrogens should be considered. Female swimmers with higher body fat percentage have a significant advantage.Growth hormone has lesser effect in both sexes (a regulator of protein synthesis).
Satellite Cells Peripheral location and activated by traumatic stress. They may provide compensatory growth of existing fibers or growth of regenerating fibers
SARCOPENIA: Loss of muscle tissueMost significant physiological change in muscle is with AGE Looking at muscles, fat and bones, we see that: At age 20, muscles are 45%, fat 20% and bones 12% of the total weight At age 75, muscles are 15%, fat 40% and bones 8% After age 49, there is a loss of 1.2 kg (3lbs) of muscle per decade
DURING SARCOPENIA: The loss appears to be more significant for the FAST FIBERS type 1 and 2 (or FO and FOG) while the SLOW FIBERS (or SO) are more stable. This fact clarifies at least in part why a 9-year-old grandson can beat grandpa easily in a 100m run but will tire much sooner in a 10km hike. Reminder: The fast fibers (normally more pale) fatigue more easily while the slow (more red) are more resistant to FATIGUE.
THE ETIOLOGY of SARCOPENIA due to a) inactivity b) decreased protein synthesis c) plus neural, hormonal and nutritional factors SARCOPENIA is aggravated: by the relative deficiency of the anabolic hormones (GH, Insulin-like GH, DHEA) BUT and AGAIN of greater importance is the DECREASE of VIGOROUS MUSCULAR WORK Any acute illness forcing elderly persons to bed rest is provoking a loss of muscle mass of about 1.5% per day Hence for 1 day of bed rest, up to 2 weeks of intense reconditioning is necessary.
Sarcopenia harder for the FAST PALE FIBERS, but why? WE DO NOT KNOW but… fiber characteristics can be modified by different modalities like hormonal administration and/or by specific exercises or activities The change in the fiber characteristic is defined as MYOPLASTICITY
MYOPLASTICITY May occur with different clinical effects, namely: -muscles enlarge with resistance type of exercise -increase their contractility (and the number of mitochondria) with endurance type of exercises -all these changes are due to stimulations and variations in the characteristics of the MYOSINS (protein isoforms)
CLINICAL significance of Myoplasticity: RESISTANCE training: increases amount of contractile proteins permitting increasing efforts. As a consequence, muscles do ENLARGE (a decrease in Ca++ concentration is needed to elicit 50% of maximal tension). • ENDURANCE training: increases the velocity of contraction, increases the number of mitochondria, and increases the capacity to oxidize substrate • Increase the Vmax (velocity of contraction) of the SO (slow) fibers • Decreases the Vmax of the FO (fast) fibers • Vmax = velocity of shortening of a fiber
BENEFITS OF EXERCISE TRAINING • (see lecture by Prof. Brooks) • Prevention of bone loss • Improvement of postural stability • Psychological benefits are to be added like preservation of cognitive functions, reduced incidence of depression and enhanced self-efficacy. • Prevention of colonic cancer possibly due to increased GI transit time and stimulation by GH and IGF-1.
CLEAR BENEFITS OBTAINED WITH EXERCISE: • Metabolic: increased insulin sensitivity and glucose tolerance. • Cardiovascular: reduces blood pressure, helps vasodilation, reduces incidence of arrythmias • Cerebral: enhanced brain blood supply and reduced episodes of thrombosis • Improved equilibrium hence fewer falls • Lower mortality rate • Higher HDL/LDL ratio
HOWEVER PROLONGED AND SEVERE EXERCISE MAY HAVE DELETERIOUS EFFECTS NOTES OF ALERT The Menstrual Cycle • Should not be disrupted • Excessive training stress and poor diet, all increase the incidence of amenorrhea. • The consequences are: infertility, premature bone loss, muscolo-skeletal injuries and scoliosis • ALL OF THESE PROBLEMS are totally preventable with planned and supervised type of exercise
TO BE AVOIDED: THE ERGOGENIC AIDS or the dreams, the failures, the tragedies THE BANNED SUBSTANCES: the DOPING CLASS 1) Stimulants like amphetamines, efedrine and even caffeine if reaching a high blood concentration 2) Beta-2-agonists like the inhalers (ventolin, albuterol and terbutaline) 3) Narcotic analgesics (or pain killers) like derivatives of morphine or codeine 4) Diuretics 5) Hormones like gonadotropin, corticotropin and erythropoietin (EPO) 6) And certain restrictions for alcohol, marijuana and corticosteroids
ALSO TO BE AVOIDED: THE ANABOLIC STEROIDS: namely testosterone but especially its derivatives manufactured to: a) minimize the sexual properties b) maximize the anabolic properties POSITIVE EFFECTS: a) increase the rate of protein synthesis b) increase strength, power and muscle size c) improve endurance capacity MAJOR SIDE EFFECTS: a) serious liver toxicity b) elevation of blood pressure c) increase levels of LDL decrease levels of HDL d) increase of the blood sugar level and in addition masculinization, increased or decreased libido, acne, depressed immune function and even psychosis
FINAL ADVICEPlenty of water Proper diet (10% protein, 25-30% fats and 60-65% carbohydrates)Liquid Cytomex or other rapidly absorbed and utilized nutrients (like Gatorade, etc.) for those wishing to enter endurance type of exercises. A DEBATED SUPPLEMENT: CREATINE!!! But still to be proven and dangerous as well (excessive hydration)