Download
1 / 22
240 likes | 470 Vues
Nursing Care & Interventions in Clients with Pituatary/Adrenal Gland Disorders. Keith Rischer RN, MA, CEN. Today’s Objectives…. Compare and contrast pathophysiology & manifestations of pituitary/adrenal gland dysfunction.

E N D
Nursing Care & Interventions in Clients with Pituatary/Adrenal Gland Disorders Keith Rischer RN, MA, CEN
Today’s Objectives… • Compare and contrast pathophysiology & manifestations of pituitary/adrenal gland dysfunction. • Identify, nursing priorities, and client education associated with pituitary/adrenal gland dysfunction. • Interpret abnormal laboratory test indicators of pituitary/adrenal gland dysfunction. • Analyze assessment to determine nursing diagnoses and formulate a plan of care for clients with pituitary and adrenal gland dysfunction. • Describe the mechanism of action, side effects and nursing interventions of pharmological management with pituitary and adrenal gland dysfunction.
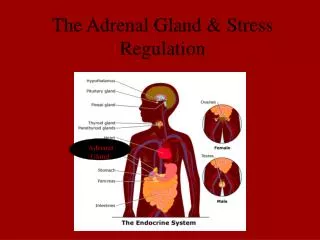
Patho: Endocrine System • Endocrine glands • Pituitary glands • Adrenal glands • Thyroid glands • Islet cells of pancreas • Parathyroid glands • Gonads • Hormones • Negative feedback mechanism
Patho: Pituitary Gland • Anterior • Growth hormone • Thyroid Stimulating Hormone (TSH) • Adrenocorticotropic Hormone (ACTH) • Follicle Stimulating Hormone (FSH) • Luteinizing Hormone (LH) • Posterior • Vasopressin • Antidiuretic hormone (ADH)
Anterior Hypo-pituitarism chart 66-1 p.1459 • Causes • Tumor • Brain or pituitary • Anorexia • Shock • Growth hormone • Gonadatropins • Women • Men • TSH • ACTH
Anterior Hypo-pituitarism • Labs • T3, T4 • Testerone, estradiol levels • Nursing interventions • Replacement of deficient hormones • Androgen therapy • gynecomastia can occur • Estrogens and progesterone • Growth hormone • Assess function of target organ • thyroid
Anterior Hyper-pituitarism • Causes • Pituitary tumors or hyperplasia • Gigantism • Acromegaly
Hypophysectomy • Post op Care • Closely monitor neuros • Assess for postnasal drip “halo sign” • Avoid coughing early after the surgery. • Keep HOB elevated • Assess for meningitis • Replace hormones and glucocorticoids as needed • Diabetes insipidus • Assess I&O closely first 24 hours
Posterior Pituitary Gland: Diabetes Insipidus • Patho • Antidiuretic hormone • deficiency • Water unable to be reabsorbed
Diabetes Insipidus: Clinical Manifestations • CV • Tachycardia • Hypotension • Heme concentration • Renal • Dramatic increased u/o • Skin • Dry mucous membranes • Neuro • Thirst • Irritable • Lethargy to unresponsive
Diabetes insipidus: Interventions • Nursing Diagnostic Statements • Deficient fluid volume r/t… • Decreased cardiac output r/t… • Priorities • Early detection dehydration • Maintain adequate hydration • Desmopressin acetate (DDAVP) intranasally • Synthetic vasopressin • I&O-daily weights
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) • Patho • Vasopressin (ADH) • Increased • Water retained • Dilutional hyponatremia • Causes • Cancer • Infection • Chemo agents • COPD
SAIDH:Clinical Manifestations • Fluid retention • Hyponatremia • Neuro • Lethargy • HA • Altered LOC • CV • Tachycardia • Renal • u/o decrease
SAIDH: Nursing Interventions • Nursing diagnostic priorities • Decreased cardiac output r/t… • Fatigue • Fluid restriction • Drug therapy • Diuretics • Hypertonic saline (3%) • Neurologic assessment • Orientation • Safe environment
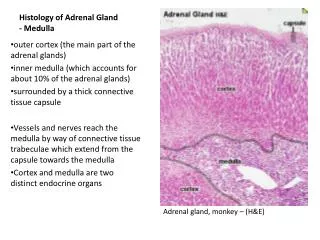
Adrenal Glands • Patho • Aldosterone • Cortisol • Catecholamines • Epinephrine • Beta receptors • Norepinephrine • Alpha receptors • Deduced aldosterone levels • Hyperkalemia • acidosis • Hyponatremia • hypovolemia
Adrenal Glands: Hypofunction • Acute adrenal insufficiency • Addisonian crisis • Causes • Steroids stopped abruptly • Clinical manifestations • Muscle weakness, fatigue, constipation • Hypoglycemia • Diaphoresis, tachy, tremors • Blood volume depletion • Hyperkalemia • cardiac arrest-rhythm changes
Addison’s Disease: Interventions • Promote fluid balance and monitor for fluid deficit. • Careful I&O • Record weight daily • Assess vital signs every 1 to 4 hours, assess for dysrhythmias or postural hypotension. • Monitor laboratory values • Na • K • Glucose • Cortisol and aldosterone replacement therapy • Diet - ↑ sodium, ↓ potassium, ↑ Carbs
Adrenal Gland: Hyperfunction • Patho • Pheochromocytoma • Cushing’s syndrome • Causes • Primary/secondary malignancies • Steroids • Lymphocytes • Inflammatory/immune response
Cushing’s Disease: Clinical Manifestations • Obesity • Changes in fat distribution • Moon face • Facial hair for women • Thin skin • Blood vessels fragile • Acne • Immunosupression • HTN • Water/sodium retention • Lab changes • Glucose • WBC • Sodium • Potassium
Nursing Priorities • Excess fluid volume r/t… • Risk for infection r/t… • Deficient knowledge
Medical Management • Drug therapy • Mitotane • If caused by side effect of medication • try to decrease or change meds • Radiation therapy • Pituitary tumors
Cushings: Surgical Management • Total hypophysectomy • Adrenalectomy • Preoperative care • Correct lyte imbalances • Postoperative care • Prevent skin breakdown • Pathologic fractures • Education regarding lifelong steroid use • Take with meals • Never skip doses • Weigh daily