Acute Appendicitis: Symptoms, Diagnosis, and Treatment
E N D
Presentation Transcript
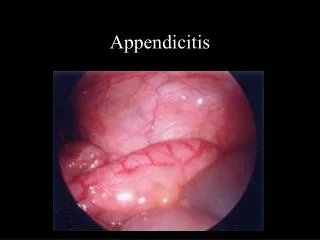
Anatomy and Function • first becomes visible in the eighth week of embryologic development as a protuberance off the terminal portion of the cecum. • The three taeniae coli converge at the junction of the cecum with the appendix and can be a useful landmark to identify the appendix.
The appendix can vary in length from <1 cm to >30 cm; most appendices are 6 to 9 cm long.
It can be found in a retrocecal, pelvic, subcecal, preileal, or right pericolic position.
the appendix is an immunologic organ that actively participates in the secretion of immunoglobulins, particularly immunoglobulin A. • Lymphoid tissue first appears in the appendix approximately 2 weeks after birth. • Although there is no clear role for the appendix in the development of human disease, recent studies demonstrate a potential correlation between appendectomy and the development of inflammatory bowel disease. • appendectomy is associated with a more benign phenotype in ulcerative colitis and a delay in onset of disease. The association between Crohn's disease and appendectomy is less clear.
Epidemiology • Despite newer imaging techniques, acute appendicitis can be very difficult to diagnose. • Peak incidence in adolescents and young adults, with a slight male predominance in this age group. • Infants, elderly, pregnant women and immunocompromised patients tend to have atypical presentations and have higher morbidity and mortality.
Incidence • The lifetime rate of appendectomy is 12% for men and 25% for women, with approximately 7% of all people undergoing appendectomy for acute appendicitis during their lifetime.
The percentage of misdiagnosed cases of appendicitis is significantly higher among women than among men (22.2 vs. 9.3%).
Etiology and Pathophysiology • Acute appendicitis is thought to begin with obstruction of the lumen • Obstruction can result from food matter, adhesions, or lymphoid hyperplasia • Mucosal secretions continue to increase intraluminal pressure
Etiology and Pathophysiology • Faecolith • Kinks • Adhesions • Worms • Gallstone • Hernia • Endometriosis • Barium • Tumour Obstruction of the lumen is the dominant etiologic factor in acute appendicitis. Fecaliths are the most common cause of appendiceal obstruction.
Pathophysiology • Exceptions exist in the classic presentation due to anatomic variability of the appendix • Appendix can be retrocecal causing the pain to localize to the right flank • In pregnancy, the appendix ca be shifted and patients can present with RUQ pain
Pathogenesis • Luminal obstruction • Bacterial stasis • Distention • Ischemia • Focal necrosis • Perforation
Bacteriology • The principal organisms seen in the normal appendix, in acute appendicitis, and in perforated appendicitis are Escherichia coliand Bacteroides fragilis. • Appendicitis is a polymicrobial infection, with some series reporting the culture of up to 14 different organisms in patients with perforation. • Antibiotic coverage is limited to 24 to 48 hours in cases of nonperforated appendicitis. For perforated appendicitis, 7 to 10 days of therapy is recommended.
History • Primary symptom: abdominal pain • ½ to 2/3 of patients have the classical presentation • Pain beginning in epigastrium or periumbilical area that is vague and hard to localize
History • In some males, retroileal appendicitis can irritate the ureter and cause testicular pain. • Pelvic appendix may irritate the bladder or rectum causing suprapubic pain, pain with urination, or feeling the need to defecate • Multiple anatomic variations explain the difficulty in diagnosing appendicitis
History • Associated symptoms: indigestion, discomfort, flatus, need to defecate, anorexia, nausea, vomiting • As the illness progresses RLQ localization typically occurs • Anorexia is the most common of associated symptoms • Vomiting is more variable, occuring in about ½ of patients
Physical Exam • Findings depend on duration of illness prior to exam. • Early on patients may not have localized tenderness • With progression there is tenderness to deep palpation over McBurney’s point • Additional components that may be helpful in diagnosis: rebound tenderness, voluntary guarding, muscular rigidity, tenderness on rectal
Physical Exam • McBurney’s Point: just below the middle of a line connecting the umbilicus and the ASIS • Rousing’s: pain in RLQ with palpation to LLQ • Rectal exam: pain can be most pronounced if the patient has pelvic appendix
Physical Exam • Psoas sign: place patient in L lateral decubitus and extend R leg at the hip. If there is pain with this movement, then the sign is positive. • Obturator sign: passively flex the R hip and knee and internally rotate the hip. If there is increased pain then the sign is positive
Physical Exam • Fever: another late finding. • At the onset of pain fever is usually not found. • Temperatures >39 C are uncommon in first 24 h, but not uncommon after rupture
Diagnosis • Acute appendicitis should be suspected in anyone with epigastric, periumbilical, right flank, or right sided abd pain who has not had an appendectomy
Diagnosis • Women of child bearing age need a pelvic exam and a pregnancy test. • Additional studies: CBC, UA, imaging studies • CBC: the WBC is of limited value. • CRP and ESR have been studied with mixed results • UA: abnormal UA results are found in 19-40% • Abnormalities include: pyuria, hematuria, bacteruria • Presence of >20 wbc per field should increase consideration of Urinary tract pathology
Diagnosis • Imaging studies: include X-rays, US, CT • Xrays of abd are abnormal in 24-95% • Abnormal findings include: fecalith, appendiceal gas, localized paralytic ileus, blurred right psoas, and free air • Abdominal xrays have limited use b/c the findings are seen in multiple other processes
Diagnosis • Graded Compression US: reported sensitivity 94.7% and specificity 88.9% • Basis of this technique is that normal bowel and appendix can be compressed whereas an inflamed appendix can not be compressed • DX: noncompressible >6mm appendix, appendicolith, periappendiceal abscess
Diagnosis • Limitations of US: retrocecal appendix may not be visualized, perforations may be missed due to return to normal diameter
Diagnosis • CT: best choice based on availability and alternative diagnoses. • In one study, CT had greater sensitivity, accuracy, -predictive value • Even if appendix is not visualized, diagnose can be made with localized fat stranding in RLQ.
Diagnosis • CT appears to change management decisions and decreases unnecessary appendectomies in women, but it is not as useful for changing management in men. Note the thick-walled and dilated appendix mesenteric streaking and "dirty fat"
Special Populations • Very young, very old, pregnant, and HIV patients present atypically and often have delayed diagnosis • High index of suspicion is needed in the these groups to get an accurate diagnosis
Differential Diagnosis • Intra-abdominal conditions • Acute Appendicitis • Acute Cholecystitis • Diverticulitis (Meckel’s) • Inflammatory Bowel Disease (Crohn’s) • Duodenal Ulcer • Intestinal Obstruction • Carcinoma of the Cecum • Nonspecific adenitis – Possible Yersinia infection
Differential Diagnosis(cont.) • Intra-pelvic conditions • Salpingitis • Pelvic Inflammatory Disease • Ectopic Pregnancy • Ruptured Corpus Luteum Cyst • Ruptured Follicular Cyst (Mittelschmerz) • Ruptured Ovarian Cyst • Ovarian Torsion • Pyelonephritis • Ureteral/Renal stone
Treatment • Appendectomy is the standard of care • Patients should be NPO, given IVF, and preoperative antibiotics • Antibiotics are most effective when given preoperatively and they decrease post-op infections and abscess formation
Treatment • There are multiple acceptable antibiotics to use as long there is anaerobic flora, enterococci and gram(-) intestinal flora coverage • Also, short acting narcotics should be used for pain management
Tumors • Primary appendiceal cancer is diagnosed in 0.9 to 1.4% of appendectomy specimens • representing >50% of the primary lesions of the appendix • mucinous adenocarcinoma (38% of total reported cases), adenocarcinoma (26%), carcinoid (17%), goblet cell carcinoma (15%), and signet-ring cell carcinoma (4%)
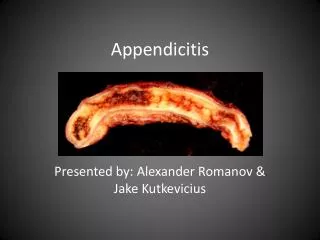
Carcinoid • firm, yellow, bulbar mass in the appendix • The appendix is the most common site of GI carcinoid, followed by the small bowel and then the rectum. • Carcinoid syndrome is rarely. Unless widespread metastases are present, which occur in 2.9% of cases.