Occupational Cancer
Occupational Cancer. Tim Morse, Ph.D. University of Connecticut Health Center, Farmington, CT, US Spring 2000. Objectives. Theoretic concerns in identifying carcinogens Estimates of occupational cancer Known exposures and occupations related to occupational cancer

Occupational Cancer
E N D
Presentation Transcript
Occupational Cancer Tim Morse, Ph.D. University of Connecticut Health Center, Farmington, CT, US Spring 2000
Objectives • Theoretic concerns in identifying carcinogens • Estimates of occupational cancer • Known exposures and occupations related to occupational cancer • Asbestos and cancer: case study • History • Risks • Control • U.S. Regulations
Issues • Multiple causation & interaction • Multiple stages • Latency period • Threshold level
Testing for Cancer • Analysis of structure-activity relations • Cell tests • Animal studies • Epidemiologic studies
Problems in testing • Prolonged high exposure is uncommon • Usually mix of exposures • Epi: expensive, long, past exposures, poor exposure data • Animal: high dose, ? Validity in humans • In vitro: mutagens, not carcinogens
How much cancer is occupational? • Doll & Peto (1981) 2-8% • Viewed as conservative • For US, 25,000-100,000 new cases/year • Higher proportions for exposed workers
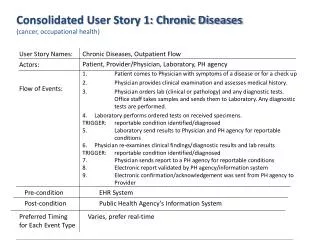
NJ Cancer Registry by Industry Excess: • Nasopharyngeal: carpenters and other blue collar special trade construction • Colorectal: machinery manufacturing, printing • Liver: general construction and rubber and plastics • Gallbladder: electrical equipment • Lung: primary metals, shipbuilding, construction, and stone, clay, and glass • Mesothelioma: shipbuilding and asbestos manufacturing
NJ Cancer Registry by Industry Excess: • Breast: (Black females) chemical and pharmaceutical • Bladder: (white males) apparel and textile industries. • Non-Hodgkin's lymphoma: • (white females) printing • (white male) bakers and motor vehicle manufacturing • Lymphocytic leukemia: chemical and construction
silica asbestos diesel engine exhaust radon progeny arsenic chromium, beryllium, nickel, and cadmium acrylonitrile Lung cancer (Steenland, 1996)
Lung Cancer Annual Incidence (Steenland, 1996) • 9,000-10,000 men • 900-1,900 women • half asbestos
Non-Hodgkins Lymphoma (Figgs, 1995) • 24 state death certificate study: 47 occupations, and 28 industries. • firefighters, • farm managers, • aircraft mechanics, • electronic repairers, • mining machine operators, and • crane and tower operators • also white collar
Women • 25% increase in lung cancer among production workers (9% decrease overall cancer) (Delzell, 1994) • Breast cancer tissue had 50-60% higher levels of DDT and PCB’s (Wolff, 1993) • 38% Breast cancer increase in electrical workers (217% for telephone installers) (Loomis, 1994)
Review of breast cancer (Goldberg, 1996) • Limited evidence: pharmaceutical industry and among cosmetologists and beauticians • Possible associations: chemists and occupations with potential exposure to extremely low frequency electromagnetic fields. • Little support: textiles workers, dry cleaning workers, and nuclear industry workers
Roofers & asphalt workers (meta analysis: Partanan, 1994) • Stomach cancer • bladder cancer • skin cancer • leukemia
Firefighters review (Golden, 1995) • leukemia, • nonHodgkin's lymphoma, • multiple myeloma, • cancers of the brain, urinary bladder, and • possibly from cancer of the prostate, large intestine, and skin.
Construction workers review (Sullivan, 1995): • Lung (70% increase from NHIS, 1988), • larynx, • oropharyngeal and nasal cancers, • mesothelioma,
Dry cleaning using perchloroethane (Ruder, 1994) • 23% increase among 20-year workers • esophogeal, intestinal, bladder
Cutting fluid exposure (Eisen, 1992) • 85% increase of laryngeal cancer (also stomach)
Occupational Cancer • IARC: ID carcinogens by worker studies • 21/22 lung carcinogens • 34/62 carcinogens overall
Overview • Background on asbestos • Uses of asbestos • Health Effects • Risk factors • Medical tests • Proper handling • Standards/ guidelines
What is Asbestos? • Mineral • Fibrous • White/grey • Indestructible • Fireproof
How Long Has it Been a Problem? • Early Greek miners wore face masks from animal bladders • Insurers stopped selling insurance in 1915 • Cancer cases in 1930’s • Asbestos industry withheld information • Selikoff studies in 1960’s • Banning of some uses in 1980’s
Uses of Asbestos • Fireproofing of buildings • Heat insulation • Strengthen building materials
Products that can contain asbestos • Spray insulation • Pipecovering • Asbestos cloth • Cements, mastic, sealants • Roofing materials • Floor & ceiling tiles • Plaster & taping compound
Hazards of Asbestos • Harmful only when breathed in (maybe when swallowed) • Fiber shape: long, thin • Travels in air, gets deep in lungs • Sharp shape gets stuck in lungs • Doesn’t break down
Asbestos Diseases • Asbestosis • Pleural Plaques • Cancer • Lung • Mesothelioma • G-I Tract
Asbestos Diseases • No completely safe levels • Higher the exposure, higher the risk • Low exposures have low risk • Everyone exposed to asbestos • Lag time (latency) of 10-40 years • No acute effects
Asbestosis • Not cancer • Scarring of lungs • From high exposures • Causes shortness of breath
Pleural Plaques • Scars on lungs • Shows up on x-rays • Marker of asbestos exposure • Half of heavily exposed will have • “Not a disease”: no symptoms • Does not change into cancer • Legally considered a disease
Lung cancer • Most common problem with asbestos • Heavily exposed workers have 5-7 times increased risk over lifetime • About same level of risk as a pack a day cigarette smoking • Interacts with cigarettes: 50-90 times increased risk for both combined • Quitting smoking reduces risk
Other Cancers • Mesothelioma • Cancer of lining of the lungs • Only caused by asbestos • Smoking not a risk factor • G-I tract cancer • 2-3 times increased risk for heavily exposed
Medical tests • Physical • History • X-rays • Lung function tests
What is Risk? • Studies are from heavily exposed asbestos workers • Construction trades working with asbestos have 1/4 or less risk than asbestos workers • Chemical plant maintenance has about 1/8 • Other maintenance workers are much lower • Asbestos has been phased out & removed in many areas
Safe handling of asbestos • Find out where the asbestos is • Management plan • Remove if needed by licensed contractors • Only dangerous if is in the air • Removal may be more dangerous than leaving • If is bound in material (tiles, etc) is not a hazard • Should be labeled if left in place
“Safe” handling of asbestos • No absolutely safe exposure • Wet methods • HEPA vacuums and respirators • Never dry sweep or compressed air • Stays in air for days • Small fibers can’t be seen • “Friable” asbestos means it can be crumbled
Maintenance & asbestos • Do not drill, sand, or saw asbestos materials • Wet mop rather than dry sweep or dust • Do not use a regular vacuum: only HEPA • Do not disturb asbestos materials • If use a face mask, only HEPA • If are air filters, use wet methods, do not shake
Training/ removal • Removal by certified contractors • Enclosures, ventilation, wet methods, HEPA • Glove bags, wetting agents, signs • Encapsulation • Training needed based on level of exposure • Level 4 for clean up of asbestos containing materials • Proper disposal while still wet; labeled bags
Regulations • EPA regulations on removal • OSHA Standard for general industry or construction • State licensing for asbestos removal • Workers’ compensation • Reporting of suspected occupational diseases
EPA:Control of Asbestos in Buildings • Survey to see if asbestos is present • Operations and Management Program • Assess the asbestos • Abatement if needed
Survey • Appoint manager & team • Check building records • Locate & document all asbestos in records • Inspect for friable • Collect & test samples • Document
Operations and Maintenance • Contact building managers & maintainers • Educate employees and occupants • Train custodians/ maintainers • Clean using HEPA & wet methods; regular basis • Special precautions for construction work • Inspect twice a year • Continue program until all asbestos removed
Assess Asbestos • Assess current conditions and chances of disturbance • Determine • Need for further action • When it needs to be done • What abatement methods to use
Conduct Abatement if Needed • Hire contractor: • To select: • Precise contract • Check references • Interview • Insurance • Best, not low bid
Managing Abatement • Inspect 4 times a day • Containment barrier • Coveralls & respirators • Changing & decontamination facilities • Stop work if problem • Release only when • Cleaned at least twice • Visual test • Airborne asbestos test
OSHA Standard • Applies if over maximum exposure • Maximum of 0.2 fibers per cc of air (8 hour) • Maximum of 1 fiber per cc (30 minute) • Exposure monitoring if above action level (0.1 fiber per cc) • Engineering controls where feasible • Proper respirators
OSHA Standard (2) • Regulated areas • Labels • Recordkeeping for 30 years • Protective clothing • Change rooms & showers • Medical Exams