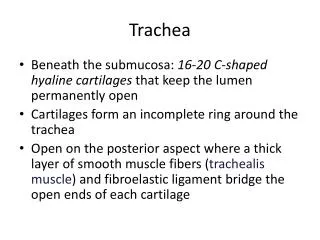
Trachea
Trachea. The MICU intern calls you at 8:15pm. Apparently, patient Johnson, who had a perc trach done several hours ago is bleeding from the trach. He is, of course, worried about a . Trachea.

Trachea
E N D
Presentation Transcript
Trachea • The MICU intern calls you at 8:15pm. Apparently, patient Johnson, who had a perc trach done several hours ago is bleeding from the trach. He is, of course, worried about a .
Trachea • The MICU intern calls you at 8:15pm. Apparently, patient Johnson, who had a perc trach done several hours ago is bleeding from the trach. He is, of course, worried about a tracheoinnominate fistula. You were signed out that the patient had a massive PE and is on heparin drip. You examine the patient, and indeed all that you see is skin oozing. What’s the next step?
Trachea (cont’d) • You check the PTT and it is > 200. After asking the MICU to lower the drip and make the PTT therapeutic, the bleeding is stopped. However, the next patient next door, who had her trach done 2 weeks ago all of a sudden has a gush of blood from her trach site. (For brevity, we will assume she has a tracheoinnominate fistula.)
Tracheoinnominate Fistula Well, doctor, what is the immediate (and definitive) treatment for this? (Think fast, the entire MICU staff is looking into the room…) Your senior and chief are in a trauma, and the nearest attending is 1 hour away.
Management of TI Fistula • Immediate • Overinflate balloon to plug hole • Stick your finger in the hole • Depress innominate artery • Definitive • Resect innominate and place graft • Leave trachea alone • Use new tracheostomy site
How to “prevent” a TI fistula • Where do you put a tracheostomy to avoid a tracheostomy? • And where exactly do you put a cricothyroidotomy?
Tracheostomy 2 to 3 rings below cricoid cartilage • Cricothyroidotomy: • through the cricothyroid membrane, above the cricoid and below the thyroid cartilage. • Ideal: #6 Cuffed • In an emergency, do not do a formal tracheostomy (even a perc trach).
Empyema • Under what conditions should you call Dr. Balaram and recommend surgical decortication? • And what are the 3 stages of natural progression of an empyema?
Empyema • Exudative phase (1st week): chest tube, abx • Fibroproliferative phase (2nd week): chest tube, abx • Organized phase (3rd week+): fibrous peel occurs around lung, chest tube unsuccessful, loculation, organization. • Needs decortication • Possible Eloesser flap, possible empyema tube afterwards
Public transportation • True story: you are standing around in the 116th Street Subway Station. Some old lady with a known huge left-sided squamous cell CA starts yakking massive amounts of blood. Assume, if you will, that this is not a GI source, nor TB (second most common source). The patient gets rushed to St. Luke’s Hospital. You are on call to the ER. What is the primary cause and what do you do?
Massive hemoptysis • > 600cc/24hrs • High-pressure bronchial arteries • Tx • Place bleeding side down • Rigid bronch to identify site if unknown • Intubate non-bleeding side of lung • Foley catheter in mainstem bronchus of affected side to tamponade bleeding • OR for lobectomy/pneumonectomy • Bronchial artery embolization if non-surgical candidate or stable
Blood supply of the trachea from all except: • Inferior thyroid artery • Internal thoracic arteries • Supreme intercostal arteries • Bronchial arteries • Recurrent laryngeal artery
Blood supply of the trachea from all except: • Inferior thyroid artery • Internal thoracic arteries • Supreme intercostal arteries • Bronchial arteries • Recurrent laryngeal artery
Which of the following does not describe the relationship between tracheal diameter and stenosis and peak expiratory flow rates? • 2cm -> 100% Peak Expiratory Flow • 10mm -> 80% PEF • 5-6mm -> 30%
Which of the following does not describe the relationship between tracheal diameter and stenosis and peak expiratory flow rates? • 2cm -> 100% Peak Expiratory Flow • 10mm -> 80% PEF • 5-6mm -> 30% • ALL OF THE ABOVE ARE TRUE.
Which of the following forms of cancer are primary and which are secondary? • Squamous cell CA • Focal, diffuse, multiple • Adenoid cystic carcinoma • Intramural and perineural spread • Laryngeal carcinomas • Bronchogenic carcinoma • Esophageal carcinoma (extension) • Thyroid carcinoma
Which of the following forms of cancer are primary and which are secondary? • Primary • Squamous cell CA • Adenoid cystic carcinoma • Secondary • Laryngeal carcinomas • Bronchogenic carcinoma • Esophageal carcinoma (extension) • Thyroid carcinoma
Which are indicators of cervical tracheal trauma? • Subcutaneous air • Respiratory distress • Hemoptysis • Pneumothorax • Persistent air leak despite chest tube
Subcutaneous air • Respiratory distress • Hemoptysis • These are indicators of mediastinal tracheal trauma • Pneumothorax • Persistent air leak despite chest tube
Which are not contraindications to tracheal repair? • Inadequately treated laryngeal problem (not unilateral vocal cord paralysis) • Need for ventilatory support or permananent tracheostomy for patients with ALS, MG, quadriplegia • Poor pulmonary reserve • Use of high-dose steroids • Inflamed recent tracheostomy
Inadequately treated laryngeal problem (not unilateral vocal cord paralysis) • Need for ventilatory support or permananent tracheostomy for patients with ALS, MG, quadriplegia • Poor pulmonary reserve • Use of high-dose steroids • Inflamed recent tracheostomy
Open lung biopsy • Sarcoidosis affects the lungs in 90% of patients with an alveolar pattern (fluffy air bronchograms) or an interstitial pattern (ground-glass or granular appearance) on CXR. Pathology reveals what characteristic finding?
Sarcoid • Non-caseating epitheloid granulomas • Bilateral hilar mediastinal lymph nodes • Skin lesions such as erythema nodosum, plaques, squamous nodules and maculopapular eruption occur in 25% • Uveitis occur in 25%
ARDS • Acute respiratory distress syndrome may be diagnosed with what typical clinopathological and radiologic findings?
ARDS • Underlying mechanism • increased pulmonary capillary permeability with extravasation of intravascular fluid and protein into the interstitium and alveoli mediated by the leukocyte • Clinical • Dyspnea • Tachypnea • Hypoxemia • Mild hypocapnea • Radiological • Diffuse bilateral infiltrates • Pathological • Vascular congestion • Alveolar collapse • Edema • Inflammatory cell infiltrate
Changes may progress to vascular thromboses and intersitial fibrosis and hyaline membrane deposits. • This leads to what following clinical findings?
Hypoxemia • Pulmonary hypertension • CO2 retention • Secondary infection • Right-sided heart failure • Hypoxia • death • PaO2/FIO2 < 200 mm Hg • Normal CO/CI • PCWP < 18 mm Hg • Non-cardiac pulmonary edema
Lung Abscesses • In the case of aspergillus, most cases may be treated with medical management and pulmonary toilet. • Name the indications when surgical therapy is warranted…
Surgical therapy Long-standing symptoms greater than 3 months before treatment Persistent cavity > 2 cm and thick walled Initial cavity > 4-6cm Failure to clear sepsis Hemoptysis Exclude dx of CA Aspergillus (fungus ball) • Treatment: • Simple drainage • Management of empyema or bronchopleural fistula • Lobectomy • External drainage • Mortality 1-5%
Clinical scenario • The 2nd year gets called to 35244-8746. This is a medical intern calling from Clark 5. The patient is an IVDU, h/o HIV, has 2 positive PPD’s, alcoholic, and non-compliant with meds. He came in 3 weeks ago with persistent hemoptysis on the MTA IRT 1 line (he got off 5 minutes before the strike started). The guys said he’s had this before up in Boston 6 months ago (he was on the Green Line then…) • What’s his diagnosis and how do you treat him?
Open positive cavity after 3-6 months of chemotherapy Resistant mycobacteria Persistent positive sputum with pathology (destroyed lug, atelectasis, bronchiectasis, bronchostenosis) amenabel to resection Negative sputum but destroyed lung, blocked cavity, tuberculoma To exclude cancer Indications for surgical treatment of tuberculosis • Localized infection with atypical mycobacteria • Tubculous bronchiectasis of lower and middle lobes (usually occurs in upper lobes – good drainage; lower and middle lobes do not drain well) • Open negative cavities if thick walled, slow response or unreliable patient • Recurrent/persistent hemoptysis (>600mL/24 hr) • Pleural disease
Actinomycosis Nocariosis Histoplasmosis Coccidiomycosis Blastomycosis Cryptococcosis Aspergillosis Mucomycosis Entamoeba histolytica The Fun-Guy’s Matching Game…(Match the extrapulmonary manifestation of the fungal infection) • Rhinocerebral, blood vessels • CNS, blood vessels • CNS • Skin > genitourinary system • Bone • Marrow, adrenal • Chest wall, CNS • Cervicofacial, chest wall • Liver abscess
Actinomycosis Nocariosis Histoplasmosis Coccidiomycosis Blastomycosis Cryptococcosis Aspergillosis Mucomycosis Entamoeba histolytica The Fun-Guy’s Matching Game…(Match the extrapulmonary manifestation of the fungal infection) • Rhinocerebral, blood vessels • CNS, blood vessels • CNS • Skin > genitourinary system • Bone • Marrow, adrenal • Chest wall, CNS • Cervicofacial, chest wall • Liver abscess Yup, they’re just in reverse order… except for the parasite…