Comprehensive Overview of Metastatic Lung Cancer Staging and Imaging Techniques
200 likes | 333 Vues
This document explains the distinctions between M0 and M1 classifications in metastatic lung cancer, outlining the absence or presence of distant metastases. It highlights the advantages of MRI over CT in assessing tumor invasion, spinal cord compression, and brain metastasis, especially for Pancoast tumors. Additionally, it discusses the role of PET scans in accurately staging mediastinal disease and detecting recurrent lung cancer. The importance of prompt diagnosis of solitary pulmonary nodules (SPN) and their characteristics suggesting benignity are also covered, emphasizing early management for potential cure.

Comprehensive Overview of Metastatic Lung Cancer Staging and Imaging Techniques
E N D
Presentation Transcript
Metastatic involvement (M) • M0 - No metastases • M1 - Metastases present
Metastases (M) • M0: No distant metastasis • M1: Distant metastasis present; or Separate tumor nodules in the ipsilateralnonprimary-tumor lobes of the lung. Separate tumor nodules in the contralateral lung are considered M1 if they are of the same histologic cell type as the primary lesion. A contralateral lung tumor with a different cell type is considered a synchronous primary lesion and should be staged independently
Advantages MRI has over CT in Tumor assessment • Mediastinal and chest wall invasion and involvement of the diaphragm. • MRI is most useful when evaluating spinal cord compression and brain metastasis . • In Pancoast tumours, invasion into the brachial plexus, subclavian artery or vertebral body by MRI has been found to be 94% accurate as opposed to 63% for CT .
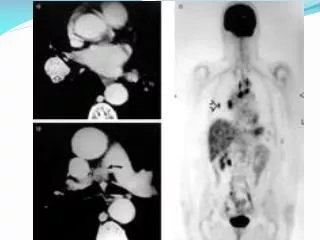
Positron Emission Tomography • PET scans appear to be more sensitive, specific, and accurate than CT scans for staging mediastinal disease. • PET is more accurate than conventional studies in detecting recurrent lung cancer. • False-positive studies do occur secondary to postirradiation inflammatory change and delaying the examination until 4 or 5 weeks postirradiation is recommended
The solitary pulmonary nodule • A common incidental CXR finding . • CT detects many more lung nodules than CXR. • Numerous differential diagnoses. • 50% are malignant: 40% are primary CA, 10% are solitary metastases . • Prompt diagnosis and management of early lung cancer manifesting as SPN may be the only chance for cure. • No significant mortality reduction with screening.
Calcification in SPN • CT scanning can further refine the detection of calcification and fat within nodules. A total 22–38% of noncalcified nodules on chest radiographs appear calcified on CT. • Eccentric or stippled calcification is seen in 10% of lung cancers.
Features of SPN suggesting benignity • Clinical history, especially of T.B. • Compared with old films,no growth over a 2-yr period. • Age <35 yrs, • No history of cigarette smoking. • No history of extrathoracic malignancy .