Download
1 / 46
460 likes | 678 Vues
Clinical Effectiveness in the Treatment of Abdominal Aortic Aneurysms. Julie Ann Freischlag, M.D. Department Director, Surgery Johns Hopkins Medical Institution Surgeon-in-Chief Johns Hopkins Hospital. IOM Definition.

E N D
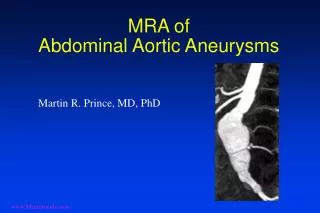
Clinical Effectiveness in the Treatment of Abdominal Aortic Aneurysms Julie Ann Freischlag, M.D. Department Director, Surgery Johns Hopkins Medical Institution Surgeon-in-Chief Johns Hopkins Hospital
IOM Definition “the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition or to improve the delivery of care.”
Patient Protection and Affordable Act 2010 Terminated Federal Coordinating Council for CER Established non-profit PCORI To identify research priorities Overseen by Board of Governors, assisted by Advisory panels CER findings may not be construed as mandates, guides or recommendations for payment, coverage or treatments
EFFECTIVENESS Represents outcomes from a treatment or health intervention in real practical settings (e.g., the real world)
EFFICACY Represents outcomes achieved from treatment or health intervention under ideal circumstances (clinical trials)
Risk Factors Abdominal Aortic Aneurysms
Abdominal Aortic Aneurysms Bernstein, AnnSurg 200:255, 1984
Impact of hospital teaching status on survival from ruptured abdominal aortic aneurysm repair Robert A Meguid MDMPH, Benjamin S. Brooke, MD Bruce A. Perler MDMBA, and Julie A. Freischlag MD, Baltimore, Maryland JVS: 2009;50:243-50
Methods • Utilized the Nationwide Inpatient Sample (NIS) file between 1998 – 2004 • Diagnosis of ruptured abdominal aortic aneurysm • Outcomes were discharge or in–hospital death and patient variables (age, gender, race and comorbidities) • Hospital level independent variables (teaching hospital, volume of open AAA and EVARfor rAAA)
Results • Of the 369 EVAR repairs, perioperative mortality was 33.3% • Mortality at teaching hospital was 26% vs 47.2% at non-TH (p<.001) • 25.2% at GSTH and 38.7% non-GSTH (p=.01) • 19.8% at VSTH and 39.0% at non-VSTH (p<.001)
Ruptured Rate of Large Abdominal Aortic Aneurysms in Patients Refusing or Unfit for Elective Repair Lederle, Johnson, Wilson, Ballard, Jordan, Blebea, Litooy, Freischlag, Bandyk, Rapp, Salam, Veteran’s Affairs Cooperative Study #417 Investigators JAMA 2002: 287:2968 - 2972
Objective: To determine the incidence of rupture in patients with large AAA in a prospective cohort study in 47 Veterans Affairs Medical Centers
Results: • 1 –year incidence of probable rupture by initial AAA diameter: 5.5 - 5.9cm 9.4% 6.0 - 6.9cm 10.2% 6.5 - 6.9cm 19.1% 7.0cm or greater 32.5% The likelihood of the AAA reaching 8.0cm during follow-up resulted in at 25.7% rupture rate in 6 months
Conclusions: The rupture rate is substantial in high–operative risk patients with AAA of at least 5.5cm in diameter and increases with larger diameter.
Rural Hospitals Face a Higher Burden of Ruptured AAA and are more likely to Transfer Patients for Emergent Repair Rubie Sue Maybury, MD, MPH1 David C. Chang, PhD, MPH, MBA2 Julie A. Freischlag, MD, FACS3 1Department of Surgery, Georgetown University Hospital 2Department of Surgery, University of California San Diego 3Department of Surgery, The Johns Hopkins Medical Institution
Objective To assess how rural hospital location influences: ● ruptured AAA presentation ● transfer after ruptured AAA ● death after ruptured AAA Elective presentation Alive AAA Admitted Rupturedpresentation Dead Transferred
Results Subject Inclusion/Exclusion Age < 50 years: 532 Traumatic aortic aneurysm: 6 Thoracic aneurysm: 22 Thoracoabdominal aneurysm: 105 Aortic aneurysm, site NOS: 8 Transferred in : 754 Rural/urban status unknown: 18,916 67,376 patients with elective AAA repair or rAAA 47,033 patients analyzed for ruptured presentation Elective AAA repairs: 40,203 6,830 patients with rAAA analyzed for transfer Transferred to an outside hospital: 148 6,682 patients with rAAA analyzed for death
Results Unadjusted Analysis
Results Unadjusted Analysis
Results Adjusted Analysis 1adjusted for age, sex, race, insurance, Charlson’s index, calendar year, 2adjusted for repair type
Conclusions • Rural hospitals face a disproportionate burden of rAAA. •Rural hospitals are more likely than urban hospitals to transfer patients with rAAA, leading to delay in repair. •For patients who are not transferred, mortality is similar at rural and urban hospitals.
Immediate Repair Compared with Surveillance of Small Abdominal Aortic Aneurysms Aneurysm Detection and Management Veterans Affairs Cooperative Study Group NEJM 2002:346:1437 - 44
Purpose: To determine if elective surgical repair of small abdominal aortic aneurysms improves survival
Results By the end of the study, 92.6% of open repair had undergone operation and 61.6% were in the surveillance group
Results: • Primary end point was death from any cause and was not significantly different in the 2 groups. (1.21, 95% confidence intervals, 0.95 – 1.54) • No reduction in rate of death related to abdominal aortic aneurysm in the immediate – repair groups (3.0%) as compared with the surveillance group (2.6%) • Mortality rate in immediate open repair was 2.7%
Conclusion: Survival is not improved by elective repair of AAA smaller than 5.5cm, even when operative mortality is low.
Two-Year Comparison of Endovascular and Open Repair of Abdominal Aortic Aneurysm Frank A. Lederle, MD Julie A. Freischlag, MD Tassos C. Kyriakides, PhD Frank T. Padberg Jr, MD Jon S. Matsumura, MD Ted R. Kohler, MD Peter H. Lin, MD Jessie M. Jean-Claude, MD Dolores F. Cikrit, MD Kathleen M. Swanson, MS RPh Peter N. Peduzzi, PhD for theOpen Versus Endovascular Repair (OVER) Veterans Affairs Cooperative Study Group
Design Multicenter randomized trial AAA ≥ 5.0 cm, candidate for both procedures Open repair vs. any FDA-approved EVR system 1º outcome = mortality
OVER Patient Characteristics • 99.3% male • 87% white • Mean age: 70 years • Mean wt: 90 kg • Current smoker: 41% • Coronary artery disease: 41% • AAA diameter < 5.5 cm: 43% ≥ 6.0 cm: 27% • EVR system: • Cook Zenith: 39%, Gore Excluder: 37% • Medtronic Aneurx: 21%, Guidant/Endologix: 3%
Other outcomes: No ruptures identified at 2 years
Conclusions: • No significant difference in the primary outcome of total mortality in this two-year analysis • Post-op mortality was lower for EVR than open, and lower for both procedures than in earlier trials. • Secondary procedures, AAA-related hospitalizations, & claudication were more frequent after EVR, but NS • No difference in major morbidities, QOL, ED • No increased late mortality after EVR by two years • Longer term data are needed to fully assess the relative merits of the two procedures