Download
1 / 23
230 likes | 244 Vues
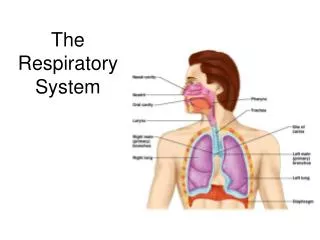
Explore how respiration and blood oxygenation are regulated, the effects of Cystic Fibrosis on lung function, and the role of surfactants in reducing surface tension in the lungs.

E N D
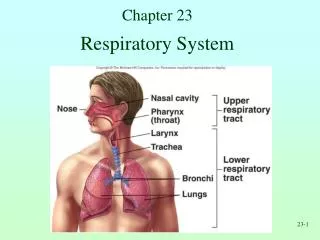
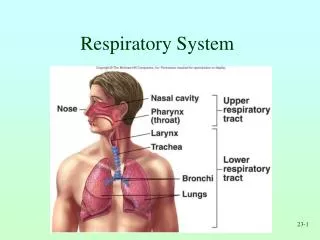
How is respiration and blood oxygenation regulated? March 22 and 25 • What is Cystic Fibrosis? • What is a ventilation-perfusion ratio? • Why do the blood vessels of the lung constrict under conditions of hypoxia? • What are some diseases that affect ventilation/perfusion ratios? • Why is it so hard to breath at high altitude? • What is High Altitude Pulmonary Edema? • What are some problems related to improper scuba diving? • How does carbonic anhydrase help us transport carbon dioxide and help us control acidosis in the blood? • What is lactic acidosis? When does it occur? How does it effect the function of the CNS? • How does the medulla control inspiration and expiration? How much voluntary control can we exert? • What happens to our control of respiration during anesthesia?
Practice Spirometry: VC=TV+IRV+ERV Assume two 5’9” peopleWhat is the Breathing Rate, TV, MRV, IRV, ERV, FVC, FEV1 and %FEV1 for each person? Which person has asthma (%FEV1) or a diminished ability to create a productive cough (based on FVC)? One Second Elapsed Time for Calculation of volume change and FEV1 during peak forced expiration
Cystic Fibrosis: What is it and why is it bad?Typically a children’s disease because they seldom lived to adulthood Genetic mutation creates a faulty epithelial cell chloride (Cl-) ion transporter. -As a result Cl- is not transported into the mucus of the lung and water does not follow the ions (sphere of hydration). -The mucus is too thick/viscous for cilia to move it (and bacteria in it) out of lung. -Spirometry: CF is both obstructive (mucous) and restrictive (tissue damage). Cycle:InfectionInflammationTissueDamageMore infection more inflammation, etc Shorter Life Span Cure: None exists except for finding a lung donor. Approach: palliative treatment only.
HOW IS TENSION CREATED/REDUCED IN THE LUNG? • Elastin in lung tissue and surfactant in alveoli both conserve energy! • Surface Tension (hydrogen bonds) of fluid lining alveoli critical • Law of Laplace: Force= 2 Tension/radius • As the radius is increased the force to inflate is reduced • Energy is required to pull volume open • Surfactant: is a phospholipid/protein mix that reduces surface tension in alveoli Critical for infants and adults alike! • Repulsion: negative repels negative • Lipid-PO4-- --PO4-Lipid • Attraction: water attached to PO4 pulls them together if they are far apart • Often premature infants lack sufficient surfactant: results in Sudden Infant Death Syndrome. • Surfactant also improves gas diffusion to/from blood
Water molecules create surface tension in the alveoli: 1) it causes small alveoli to collapse, and 2) it causes air to be diverted to the larger of any two alveoli because larger alveoli are easier to keep inflated. Surfactants are phospholipids that help prevent complete alveolar collapse due to the compaction of strong opposing negative charges on the phosphates! Surfactants also provide elasticity to help the lung work passively, adding to the effect of elastin proteins found in the lung tissue!
What is alveolar ventilation? When you inspire the diameter/size of trachea, bronchi and bronchioles does not change much. • You have about 300 million alveoli, they never want to completely collapse (surface tension vs surfactant) • When you inspire, air inflates individual alveoli. The more you inspire, the greater the number of alveoli filled (recruitment) • Peak inspiration (IRV) =the maximum number filled with air • Alveolar ventilation: Liters, milliliters, or expressed as %TV • ….larger breath…greater percent of breath found in alveoli. TidalVolume(0.5L)-DeadSpace(0.35L)=AlveolarVentilation(0.15L) Alveolar Ventilation is about 30% of a TV at rest, 40% of a TV during moderate exercise, 70% of TV during large tidal volumes
What terms describe a person’s breathing pattern?Vocab/Reference values to know for test #3 • Know approximate values for VC, TV, IRV, ERV and RC for a typical 157 pound person. • Typical Values: VC(5L), TV(0.5L), IRV(3L), ERV(1.5L) and RC (1.0L) • Normal Respiration: 12 bpm @ 500 ml TV • Normal MRV= TV X Breathing Rate • Typical MRV= 500ml/breathX10 breaths/minute = 5 L/min • Typical gas pressures (mmHg) in airways and blood • Eupnea: quiet normal TV • Dyspnea: Sense of shortness and gasping • Apnea: breathing temporarily stops • Respiratory Arrest: Full stop • Hypernea: Increased rate • Hypoventilation: Breath too slow • Hyperventilation: Breath to fast • Breaking Point: when you cannot voluntarily breath hold any more
Gas partial pressures are very important to consider, especially for those who may work with anesthesia in the future! Total P=760 mmHg: N2=597, O2=159, H2O=3.7 and CO2=0.3mmHg. Alveolar Air Partial Pressure: N2=569, O2=104, H2O=47 CO2=40mmHg. Test Question for Test#3: Fill in the blanks with the correct partial pressures.
Hemoglobin in blood that passes through gas-exchange regions of the lung (alveoli/respiratory bronchioles) is RAPIDLY oxygenated to 100% saturation
Ideally we want about 4.2L of air to enter the lungs for every 5.5L blood passing through the lungs (4.2/5.5 is a ratio of about 0.8). Ideally the blood only goes to the parts of the lung that are ventilated.
Blood vessels in the lung vasodilate in response to a very different set of conditions than systemic circuit. Vascular Smooth Muscle in Arteries in Systemic Circuit: • 1) If blood vessels dilate resistance decreases and flow can increase. • 2) In the systemic circuit, hypercapnia means high metabolic activity level and high oxygen needs. • 3) In the systemic circuit hypercapnia causes vasodilation to improve blood flow, O2 delivery, and CO2 removal at local areas of need. The Arteries of the Lung Respond VERY Differently! (REVERSAL) • 1) Any time low oxygen levels are detected it means the lung has no ability to oxygenate blood sent to this region. (collapse or infection?) • 2) Hypoxic pulmonary arterial smooth muscles vasoconstrict so blood does not perfuse areas with no ability to oxygenate blood. • 3) Blood vessels dilate in regions of the lung that have oxygen. • 4) This means blood only passes to regions of the lung that have oxygen and blood is not sent to Non-ventilated regions.
Ventilation of air and perfusion of alveolar capillaries with blood should be at about a 1:1 ratio (4.2/5.5=0.8 to be exact). CONSIDER EFFECTS OF atelectasis, pneumonia, and aspirated objects.
What are the tricks to prevent sending blood to alveoli with too little air (oxygen) due to atelectasis or obstructed airways, or to alveoli where gases in air can’t reach the blood (pneumonia). How does gravity (1.92 mmHg/inch) limit perfusion at the top of the lung?
How does high altitude affect total atmospheric pressure and the partial pressure of oxygen in the air? Data we collected in India in 2004
If the partial pressure of the oxygen in the air decreases, the partial pressure in the alveoli should decrease, and then the hemoglobin saturation should also decrease…and it does!What effect would this have on your ability to do exercise?
Why is High Altitude a Partial Pressure/Gas Exchange Problem? Total Gas Pressure Total at High Altitude is Reduced • H2O vapor stays 100% saturated in alveoli (47 mmHg)! • There are fewer mmHg of partial pressure left for oxygen! How would you expect the breathing rate and tidal volume to compensate for the mild hypoxia? Why is there a High Risk for dehydration at high altitude! Development of High Altitude Pulmonary Edema (HAPE) is a problem related to inappropriate vasoconstriction and increased pulmonary arterial resistance causing edema in lung. Edema promotes a positive feedback loop and death. Sometimes this is called “death breathing” in hospice care or nursing home after a massive left side heart attack.
There were tragic consequences for the fellow with the bottle because he failed to respect the effects of altitude.His %SpO2 was 49% and his heart rate was 169 BPMWould this be normal for a person with HAPE? Why?
This poor fellow had HAPE so bad that when he exhaled it sounded like he was breathing out through a tiny straw underwater! Having been like this for 3 days untreated, his blood vessels were rapidly constricting in all parts of his lung. Where did the water go? EDEMAThe poor fellow died a few hours later after being carried further down the mountain of massive pulmonary edema.
RESPIRATORY PROBLEMS AND SCUBA DIVING. Scuba Troubles: Atmospheric pressure much greater than 760 mmHg! • Nitrogen gas present in blood at MUCH greater that 560 mmHg…while under water! • Problem: When you come to the surface the nitrogen gas come out of solution as gas bubbles in joints and spinal cord….EXTREME PAIN! • THE BENDS: DECOMRESSION SICKNESS! • Treatment: Hyperbaric Chamber Why did Dr. Wilson’s student have trouble scuba diving, drinking and flying home from Cancun on the same day? OUCH! Other Possible Scuba Problems: • Nitrogen Narcosis (“Rapture of the Deep”)- • Breath hold ascent and pulmonary barotrauma-
CO2 solubility in the blood is (like oxygen) very limited, so we: 1) Reversibly convert it to bicarbonate with CA (70%)2) Carry it on deoxygenated Hb molecules in RBCs (23%)3) Let it move freely dissolved in blood (7%). Hint: This (fill-in-blank) will be on Test #3.
THE MEDULLA IS THE CENTER OF AUTONOMIC BREATHING CONTROL. Responsibilities include: INHALATION: Inspiratory (DRG) “On”/ Expiratory (VRG) “Off”: EXHALATION: Turn “Off” Inspiratory center (DRG) and use good ol’e passive elastic recoil!…..Activation of VRG can provide extra forced expiration via contraction of internal intercostal muscles! • Medulla detects plasma PROTONS (H+) from pCO2 (very sensitive) and physiologic activity (proprioception). The medulla adjusts inspiratory/expiratory center activities as needed based on these inputs! Detection of low arterial pO2 • Prevention of excess inspiration: Herring-Bauer Reflex/Vagus • Provision for voluntary respiratory control: Breath Holding vs. Breaking Point (Medullary Over-ride) • Over All: Understanding of the interplay of these mechanisms is poorly understood.
+DRG: Inspire Turns off VRG! Contraction of: Ext. intercostals and diaphragm +VRG: Expire Turns off DRG! Passive Relaxation Or Contraction of: Int. intercostals VIP: T1-11: Vertebral nerves to intercostals VIP: C3-5: Phrenic nerve to diaphragm Final action potentials that control respiration are sent out of the medulla, however the pons can also send stimulatory or inhibitory input to the medulla.
What are some important changes that can occur in respiration during anesthesia? • Cheyne-Stokes Breathing Pattern and alcohol/anesthesia: detection of oxygen as last stimulus for inspiration in brain. • Choppy breathing pattern gets deeper and deeper as barbiturate effect on brain deepens • Anesthesia and irritation of stomach lining: • Anesthesia and glottic adductor muscles • Vomiting in absence of closed glottis does what? • Why was a intratracheal tube place prior to surgery? • Where is your cough reflex? • What happens if you cannot cough? • What happens if Pons and Medulla can’t to detect H+ and O2?