Download
1 / 35
420 likes | 1.13k Vues
We cannot teach people anything; we can only help them discover it within themselves. Galileo Galilei. Introduction to Respiratory system Structure and Function of the Respiratory System. Learning objectives. Physioanatomy of the upper and lower respiratory tract Weibel model

E N D
We cannot teach people anything; we can only help them discover itwithin themselves. Galileo Galilei
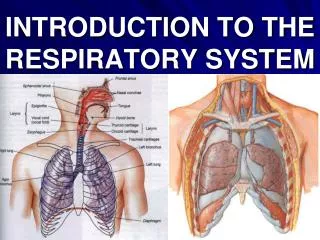
Introduction to Respiratory systemStructure and Function of the Respiratory System
Learning objectives • Physioanatomy of the upper and lower respiratory tract • Weibel model • Air flow and factors affecting airway resistance. • Innervation and blood supply of the lung. • Lung defence mechanism. • Metabolic ,endocrine and other functions of the respiratory system.
Upper Airways-Nose, Sinuses, Larynx ,vocal cords • The major function of the upper airways is to "condition" inspired air so that by the time it reaches the trachea, it is at body temperature and fully humidified. • The nose -filter, entrap, and clear particles larger than 10 μm in size. • Nose provides the sense of smell. • Resistance to airflow in the nose during quiet breathing accounts for approximately 50% of the total resistance of the respiratory system.
The sinuses lighten the skull, which makes upright posture easier, and they offer resonance to the voice. • The major structures of the larynx include the epiglottis, arytenoids, and vocal cords . With some infections, these structures can become edematous (swollen) and contribute significantly to airflow resistance. • The epiglottis and arytenoids "hood" or cover the vocal cords during swallowing.
Lower Airways-Trachea, Bronchi, Bronchioles, Respiratory Unit
IN THE CLINIC • Asthma involves both large and small airways and is characterized by inflammation, predominantly mediated by lymphocytes and eosinophils, in the airways and reversible airway smooth muscle constriction (bronchospasm). • Bronchiolitis is a disease of the small airways. It usually occurs in young infants and is caused by viruses, most commonly respiratory syncytial virus. • Chronic bronchitis, a disease of smokers, is associated with a marked increase in mucus-secreting cells in the airways and an increase in mucus production.
Airflow in Airways Two major factors determine the speed at which gas flows into the airways for a given pressure change: • the pattern of gas flow- laminar/turbulent • resistance to airflow by the airways.
Reynolds number (Re) • The Reynolds number (Re) is a dimensionless value that expresses the ratio of two dimensionally equivalent terms (kinematic/viscosity). • where d is the fluid density, v is the average velocity, r is the radius, and η is the viscosity. • In straight tubes, turbulence occurs when the Reynolds number is greater than 2000.
Airway Resistance • (Q = ∆P/R). Resistance is determined by Poiseuille's law
The medium sized bronchi are the sites of highest airway resistance. • smallest airways are arranged in parallel [total resistance is less than individual resistances] and the total cross sectional area for smallest airway is greater than that for medium sized bronchi.
Neuro-humoral Regulation of Airway Resistance AIRWAY DILATION AIRWAY CONSTRICTION Stimulation of efferent vagal fibers, either directly or reflexively (smoke, dust, cold air, or other irritants ) Agents such as histamine, acetylcholine, thromboxane A2, prostaglandin F2, and leukotrienesreleased by airway cells in response to various triggers, such as allergens and viral infections • Stimulation of the sympathetic nerves and release of the postganglionic neurotransmitter norepinephrine
BLOOD SUPPLY TO THE LUNG PULMONARY CIRCULATION BRONCHIAL CIRCULATION The bronchial circulation arises from the aorta and contains 1% to 2% of cardiac output They nourish the walls of the bronchi, bronchioles, blood vessels, and nerves, and they perfuse the lymph nodes and most of the visceral pleura • The pulmonary circulation brings deoxygenated blood from the right ventricle to the gas-exchanging units for removal of CO2 and oxygenation before blood is returned to the left atrium for distribution to the rest of the body.
Lung Interstitium • Fibroblasts-synthesize and secrete collagen and elastin • Collagenis the major structural component of the lung that limits lung distensibility. • Elastinis the major contributor to elastic recoil of the lung. • Cartilageis a tough, resilient connective tissue that supports the conducting airways of the lung and encircles about 80% of the trachea. • Kultschitzky cells, neuroendocrine cells, are found in clumps throughout the tracheobronchial tree and secrete biogenic amines, including dopamine and 5-hydroxytryptamine (serotonin).
Lung Defense mechanisms: • Removal of Particles – by hairs of nostrils • particles of 2 – 10 microns in diameter are removed by cilia – ciliary escalator; • Particles less than 2 microns in diameter are removed by pulmonary alveolar macrophages (dustcells)].
Mucociliary Escalator The cilia are bathed in a periciliary fluid . On top of the periciliary layer and the beating cilia rests a mucus layer, a complex mixture of proteins and polysaccharides secreted from specialized cells, glands, or both in the conducting airway. This combination allows for the trapping of foreign particles (in the mucus) and their transport out of the airway (powered by ciliary beat)
Cystic fibrosis • Is a genetically inherited disease that adversely affects chloride channels in exocrine glands. • Faulty regulation of Na+ absorption and inability to secrete Cl–reduce the volume of liquid on airway surfaces; i.e., they are "dehydrated." • Both the thickening of mucus and the depletion of the periciliary liquid lead to adhesion of mucus to the airway surface. • Mucus adhesion leads to a failure to clear mucus from the airways both by ciliary and airflow-dependent (cough) mechanisms. • This results in a reduced periciliary layer that inhibits function of the mucociliary escalator, and alters the local environment to reduce the effectiveness of antimicrobial secretions.
Airway epithelial cells- produce • Secretory immunoglobulins (IgA), • Collectins(including Surfactant A and D), Defensins • Peptides and proteases, • reactive oxygen species, and reactive nitrogen species
functions: contd • Blood reservoir • lyses of clots in pulmonary vessels. • Small thrombi are filtered. • Plays a role in clotting mechanism – mast cells contain heparin. • Excretion of volatile substances – ketone bodies • Helps in Phonation • Regulation of body temperature • Regulation of water balance • Regulation of acid base balance