DIAGNOSING LYME WITH MS FEATURES
200 likes | 218 Vues
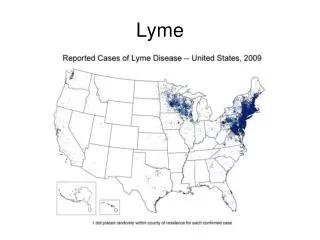
This resource explores the challenges in diagnosing Lyme disease with features overlapping MS, highlighting treatment strategies and diagnostic criteria. Discover case studies with treatment summaries, lab data, and patient histories.

DIAGNOSING LYME WITH MS FEATURES
E N D
Presentation Transcript
Steven J. Harris, MD DIAGNOSING LYME WITH MS FEATURES
Introduction • Diagnosis • Issues Particular to Lyme • Case 1 • Case 2 • Case 3
Introduction • Lyme disease has several neurologic features overlapping with MS. • Not only is diagnosis challenging, but once the diagnosis is established, treatment strategies remain unclear. • How do we create a best practices model to diagnose Lyme with MS features? • Are there any new, useful treatment strategies to include in the various antibiotic regimens?
Discreet episodes in space and time • 2 clinical attacks originating from • separate lesions, lasting at least 24 hours. • 3 months must separate the discreet • attacks • MRI 4 white matter areas of increased • signal intensity at least 3mm diameter • CSF oligoclonal IgG bands different from • any such bands in serum • Elevated IgG synthesis/index (90%) • Elevated myelin basic protein (80%) • Elevated neurofilament levels • Normal aldolase levels • Normal CSF lymphocyte levels (66%) • Ab to oligodendrocyte-glycoprotein MS VS. LYME MS LYME • Borrelia Burgdorferi IgM, IgG,IgA Ab • Pleocytosis • Elevated CSF protein • Kynurenines • Some matrix-metalloproteinases • Dendritic cells-plasmacytoids Sources: Schmutzhard, Erich, Multiple Sclerosis and Lyme Borreliosis; Winer Klinische Wochenschrift; July 31, 2002 International MS Support Foundation
Lab Data + + + + Tests Lyme MS • IgG syntesis rate • myelin basic protein • Oligoclonal IgG Bands • Anti-Neuronal Nuclear Antibody (ANNA), IFA/WB • Lymphocytic pleocytosis • Specific antibody • DNA/antigen/organism detection • CSF elevated protein + + + +/-
Problems With Diagnosis Test/Criteria Actual Practice/Assumptions • CSF Lyme PCR • Urine PCR probably more reliable • CSF Lyme Antibody • Often not present, despite literature • MRI • Changes over time/ rigid criteria not able to distinguish • SPECT • MRS • Data lacking in Lyme What are the criteria to diagnose Lyme in the absence of Laboratory evidence?
TREATMENT SUMMARY Symptoms gone after Dr. Shantha program. Fatigue better. No neuropathy. Memory more precise. PLAN: Hold antibiotics. Zhang’s herbs if desired. Vitamins, diet, heat, rest and sunlight. In 3 mos ABX Challenge and urine LDA/PCR Oral antibiotics for for several months. IV for 10 days. Poor tolerance of IV. Presumed to be JH rxn. Pt 3 On Tegretol, refusing tinidazole or metronidazole; zithromax precluded. Intense fear over recurrence of seizures. Environmental allergy gone, spinal dysesthesia absent. Executive functioning now decaying again after a long course to resolution. Patients with features of MS, undergoing treatment for Lyme. Fighting Insurance companies for treatment. Now on Ceftriaxone 2g qd X 10 months. Pt 2 Pt 1 Hx Dr. Ling’s program. Doxy tid x 4 years and Biaxin 500 bid x 4 years. Plateau until one month ceftriax. All symptoms gone x 2 months. Insurance denial Incontinence recurred. Near syncope x several. Awaiting pregnancy. Restarting orals x 1 week.
Laboratory History Pre-treatment Exam Post-treatment Exam • LUAT 152 7/00 • WB 09/00 IgM 30,31, 58,66 IgG 30, 41, 58 • urine pcr + 4/01 • urine pcr + 6/02 • Babesia serology neg • Deer tick San Diego 1995. Given Doxy x 1 week. 1 month later unable to walk; vision deteriorated • Dx’d MS by MRI/neurologist 1996. • Told no Lyme in California and offered hymenoptera shots. • Diagnosed Lyme by Dr. Ling 1996 • Presented 08/01 with incontinence, imbalance, syncope,fatigue, clumsiness, sweats, hair loss, heart palpitation • left foot edema • impaired finger/nose • +romberg • poor tandem gait • speech slurring • hypesthesia fingers/toes • muscle twitching • bilateral Lower extremity weakness • Full strength • all findings normal except slight tandem gait difficulty and slight sensory deficit in fingers Patient 1 • Treated 4 years with zovirax, Doxy, Biaxin. Vision returned after 2 years. Plateaued. • Off meds x 2 months in 2000. • Previous gains diminishing • Started on Ceftin and Flagyl (pulsed) x 9 months. Improved, then plateaued. Switched to Amox due to Ceftin cost. No change. • Off meds x 3 months in 2001 • 8/01 Started Biaxin 500 BID, Ceftin 500 BID, Plaquenil 200 BID. Added 4 g Amox for 6 days monthly during Herx. Modest response. • Started Ceftriaxone 2g/day 11/01. Flare 10 days later; then definite, progressive response. • 12/01 returned to work, driving
On Rocephin x 6 months, finishing 05/02. After 4 months on IV nearly all symptoms gone. No meds x 1 month. Felt fine. Urine PCR + 06/02. Amox restarted 875 qid. Pt presented 10/02 with recurrence of venous lakes under eyes Recurrence of syncope, urinary incontinence right foot drop, +romberg, moderate sensory neuropathy left toes Tandem gait worse than pretreatment Patient 1 Plan: restart Tinidazole 500 tid. Continue Amox. In 2 weeks begin Biaxin 500 bid. In 6 weeks add plaquenil 200 bid. If no response in 10 weeks, or if worse, resume Rocephin x 12-15 months. Counfounder: pt wants to get pregnant. Averse to more IV abx.
PATIENT 2 41 yo law enforcement officer. Questionable tick bite right hand 05/98 in Pasadena/Los Angeles . Diagnosed as ringworm. By 10/98 developed Bells palsy, visual disturbance, head pressure, vibratory sensation in spine, weakness, severe imbalance diplopia. Developed acral numbness and dysesthesia. Symptoms sporadic, coming and going every few days with variable severity. 11/98 joint pain, head numbness, brain fog, myoclonic jerks. 03/99 Started Tegretol 225 tid. Diagnosed probable remitting/relapsing MS and partial complex seizures 4/99. Brief trial of interferon-beta. No change. Diagnosed Lyme Disease 10/00. Declined IV Rocephin. Began Amox 1g tid 01/01. Within one week, neurological problems improved. Soon developed several round rashes on legs and hands and cramping in legs.Despite recommendations from her primary Lyme doctor and myself patient did not begin more intensive therapy (ie. Tinidazole). Developed tremendous environmental allergies and headaches. 03/02 Commenced Rocephin 1g bid (per patient request). Had significant flare in musculoskeletal symptoms lasting 6 weeks. Allergies improved. By 05/02 had vibration in arms, neck stiffness, light-headedness. 06/02 Biaxin added. Seizure-like activity resulted in discontinuation. Hospitalized for several days for spinal vibrational pain. With high dose magnesium, resolved in 1 day. 07/02 no further spine or peripheral nerve pain. Started experiencing monthly flares of myalgia, neck stiffness,muscle spasms. 09/02 spine tingling recurred. Food allergies recurred. However, muscle mass greatly increased. Overall looked stronger. 11/02 allergies recurred. Fatigue improved. Hypomanic. Severe cognitive decline in two months. Refusing to attempt zithromax, metronidazole, tinidazole or any other anti-seizure medicine. Fear of doctors and unable to follow advice.
PATIENT 2 Initially patient doing better on Rocephin Started Declining after 7 months. Recent (10/02) neuropsychological evaluation gave her a GAF of 4.5
10/98 CSF protein 36 wbc 13 87% lymphs 13% monos. Myelin Basic Protein (MBP) 1.3 ug/L (wnl) IgG syn 22.7 mg/d (hi) +oligoclonal bnds 01/99 CSF MBP 1.3 IgG syn 17.1 +oligoclonal bands 11/99 CSF MBP <0.5 IgG syn 18.8 oligoclonal bnds negative Lyme Ab IgM IgG IFA neg 01/02 CSF protein 33 wbc 0 lymphs 12 MBP 1.2 IgG syn 32.1 oligoclonal bands 3-4 12/98 Lyme ELISA neg 05/99 Lyme ELISA pos 10/00 LUAT 40 172 38 (pos) 12/00 Lyme WB IgM 30, 39, 45, +/-66 IgG 30,41,45 (Igenex) 05/01 Lyme WB IgM 18,37,39,41,45,66; IgG 30,+/-39,41,45 08/01 Lyme ELISA pos x 2 08/01 Lyme WB IgM 18, 39,41,45 IgG 30,+/-39,41,45, +/-58,+/-66 (Igenex) 08/01 Lyme PCR whole blood neg x 2 08/01 LDA (urine) pos 2/3 PCR urine neg 01/02 Lyme WB IgM 41 IgG 41 (Stony Brook) 01/02 Lyme WB IgG neg IgM neg (FOCUS) PATIENT 2 LAB DATA
Patient 2 Lab Data • Electrolytes consistently normal • CBC consistently normal • sed rate occasionally mildly elevated • Babesia PCR neg, IgM equivocal x1; neg x 2, IgG equivocal x1;neg x1; pos x 1 • HME IgM equivocal x1; IgG neg x1 • Bartonella neg • ANA neg • anticardiolipin Ab negative >10 times
Patient 2 Radiology- MRI BRAIN • 10/98 increased signal intensity in white matter bilaterally • 03/99 no change. “A few Multiple Sclerosis plaques are seen in the periventricular region” • 01/00 a few small punctate areas. Less than previous exam • 06/00 No increased signal intensity areas seen as evident on previous. • 11/01 a few scattered periventricular white matter signal abnormalities • 03/02 scattered periventricular white matter signal abnormalities consistent with demyelination • 08/02 SPECT BRAIN moderately diminished perfusion in frontal/orbitofrontal regions as wellas at temporal lobe tips and left temporoparietal region • 10/02 multiple periventricular signal abnormalities worse on left side. Worse over previous exam
Patient 2 MRI SPINE • 08/99 lumbar L4 bulging disc. O/w normal • 07/01 cervical areas of increased T2 signal in cervical and thoracic spinal cord • 11/01 thoracic patchy cord signal T3-T7 right side • 03/02 cervical abnormal contrast enhancement C2-C5. Mild cord expansion. “Most likely etiology is MS” • 09/02 cervical resolution of cord expansion at C2-C5. Less signal abnormality • 09/02 thoracic minimally improved patchy signal changes
27 yo female undefined bug bite on right thigh November, 1998 in San Fernando Valley (Los Angeles County). Two weeks later myalgias, fatigue, headaches, balance problems. Soon after developed tingling in arms, ear pain and visual disturbance. Initially diagnosed with depression. Placed on prozac. No change. Seen by neurology for r/o MS. 02/99 LP negative for protein, MLB, oligoclonal bands and Lyme antibodies. MRI negative. Found to have positive Lyme ELISA by Kaiser ID. Placed on Doxycyline 100 bid x 28d despite being told Lyme was doubtful “no Lyme in California”. Symptoms resolved until March, 2001 when she developed severe balance problems, memory loss, unilateral facial numbness and diplopia, sensory neuropathy in legs and feet. Patient 3
Repeat serology +Lyme. WB (AML-Kaiser) negative. Told she did not have Lyme, but placed on Amoxicillin x 2 weeks 12/01 and then Ceftriaxone, planned for 21 days. After 3 days, felt better. One week later, developed rash and fever, taken off Ceftriaxone and placed on Doxy for 1 week. Repeat LP negative. Over next 6 weeks while off meds symptoms got gradually worse. Seen 2/02. Had hyperreflexia and left foot sensory neuropathy. Babesia serology, WA-1, Erlichea serology neg. Lyme IgG Bands 23-25, 28, 30, 31, 41. IgM Bands 18, 30, 45, 58, 93. Started Amox 875 tid x 4 months and Flagyl 6 weeks on 3 months off. Zithromax added 6/02. All symptoms resolved except memory. Dr. Zhang’s herbs x 2 months. August,2002 to Dr. Shantha x2 weeks. Currently all symptoms resolved, including memory. Patient 3
Summary of Issues Patient 1 Patient 2 Patient 3 • Risks of therapy • Costs of therapy • Long term outcomes • unclear • Next steps? • MRI worse after treatment • Treatment not complete • Pt getting worse again, despite • 10 months Rocephin. Presume • cystic forms. • How long to treat? • Restart IV antibiotics • now?
Towards a Best Practices Model in Diagnosing Lyme With MS Features Lyme Disease Laboratory, Radiological, Clinical Multiple Sclerosis
Towards a Best Practices Model in Treating Lyme With MS Features Lyme Disease Antibiotics Heat Hyperbaric O2 Intracellular Facilitators Diet/ Supplement Immune modulation Homeopathy energy work other... Symptom Resolution/Cure