Spirochetes & Gram Negative Cocci
Spirochetes & Gram Negative Cocci. Professor Sudheer Kher. Learning Objectives. Enlist medically important GNCs & Spirochetes List important virulence factors Describe the mechanism of development of infection by GNCs List pathogenicity of meningococci & gonococci

Spirochetes & Gram Negative Cocci
E N D
Presentation Transcript
Spirochetes & Gram Negative Cocci Professor Sudheer Kher
Learning Objectives • Enlist medically important GNCs & Spirochetes • List important virulence factors • Describe the mechanism of development of infection by GNCs • List pathogenicity of meningococci & gonococci • List spirochetes and diseases caused by them • List Lab tests for diagnosis of syphilis Resources - Ananthanarayan Ch 25, 42
Spirochete Axial filament Treponema pallidum Syphilis Chancre Primary lesion Darkfield microscopy Secondary Lesion Tertiary Lesion Anti-cardiolipin antibodies VDRL/RPR tests Borrelia burgdorferi Lyme disease Relapsing fever Vincent’s angina Leptospira (leptospirosis, Weil’s Disease) Neisseria Thayer Martin medium N. gonorrhoeae Gonorrhea N. meningitidis Meningitis Fulminant meningococcemia Key Words
SPIROCHETES Treponema, Borrelia and Leptospira
Spirochetes • Gram negative • Long, thin, helical, motile • Axial filaments • Locomotion • Between peptidoglycan layer/outer membrane • Runs parallel
Treponema pallidum • Transmission • genital/genital • in utero or during birth • Pathogenicity • Syphilis • Chronic, Slowly progressing
Primary lesion • - chancre • 10 to 60 days • area of ulceration & inflammation • many organisms • Secondary (2-10 weeks later) • systemic spread • flu-like symptoms • skin, particularly • many organisms • Tertiary • several years later • rare • skin, central nervous system • delayed hypersensitivity • few organisms • control by immune response Syphilis
Microbiological diagnosis • Not culturable • Dark field microscopy • Actively motile organisms • Brightly lit against dark backdrop • Light shines at an angle • Reflected from thin organisms • Enters objective • Silver impregnation Fontana / Levaditi stain • Fluorescence microscopy antibody staining
Secondary and Tertiary Syphilis- serology • Screening method • Antibodies to cardiolipin VDRL / RPR Tests • False positive result possible • Specific diagnosis • Antibodies to treponemal antigen TPHA • No false positives • Once positive remain so for many years.
Borrelia burgdorferi and Lyme disease Ixodes scapularis, tick vector for Lyme disease. Also known as Ixodes dammini. CDC Lyme Disease erythematous rash
Lyme disease - symptoms • bacteremia • acute • arthritis • cardiac • neurologic • chronic • weeks, months later Atick bite leads to transmission of B. burgdorferi
Therapy • Early antibiotic therapy • Curable • Penicillin • Tetracycline • Late antibiotic administration • Ineffective
Diagnosis A physicians dilemma • Serum antibodies to B. burgdorferi. • Laboratory strains • Grow extremely slowly • Tissue culture media • Not bacteriological media • Patient body fluids/tissue sample • Almost never growth • Acute • responds to antibiotic • antibodies not detectable • Late diagnosis • not curable • antibodies detectable
Relapsing fever Diagnosis • Transmission • Lice-B. recurrentis • Human, primary host • Immune response develops • Fever disappears • New antigens expressed • No immunity • Disease reappears • No culture • No serological test • Detected - blood smear
Borrelia vincentii • Extremely painful condition of oral cavity • Symbiotic infection with Fusobacterium fusiformis • Normal inhabitant of mouth • Can cause Vincent’s Angina
Leptospirosis • Symptoms • flu-like • severe systemic disease • Liver • kidney • Brain • Eye
Transmission • Infected urine • rodents • farm animals • Water • Through broken skin.
Laboratory Diagnosis • Serology • Most readily culturable of spirochetes • culture still extremely difficult
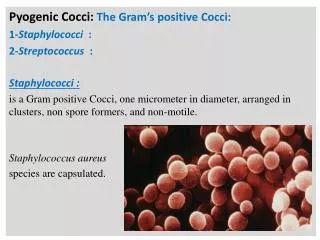
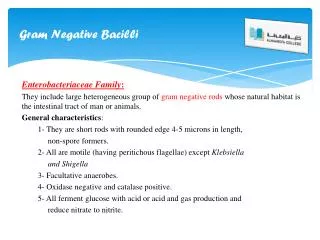
Neisseria • Gram negative • Diplococci (pairs of cocci) • Oxidase positive • Culture • Thayer Martin. • selective • chocolate agar • heated blood (brown)
N. gonorrhoeae the “Gonococcus" • Exclusive disease of humans • Gonorrhea • Urethritis in men • Endo-cervicitis in women • Second most common venereal disease • Ophthalmia neonatorum – Non venereal transmission • Crede’s prophylaxis – Silver nitrate eye drops
Smear • Polymorphonuclear cell • Gram negative cocci • Many in cells
Dissemination -gonococci • Gonoccocal arthritis • “septic” arthritis • Dermatitis
Antibiotic therapy • βlactamase-resistant cephalosporin • e.g. ceftriaxone • resistant strains • common • produceβ lactamases • destroy penicillin
Pathogensis • Adhesion to genital epithelium • Outer membrane • Pili (Fimbrae) • Antigenicity • highly variable among strains • No vaccine • IgA protease • also N. meningitidis
N. gonorrhoeae • Tissue injury • lipopolysaccharide • peptidoglycan • OnlyFimbriated strains cause disease
N. meningitidis • Resides in humans only • Usually sporadic cases • mostly young children • Outbreaks • Adults • Crowded conditions • e.g. Army barracks, Dorms
Neisseriameningitidis • Upper respiratory tractinfection • Adhesion pili • Bloodstream Brain
Meningococcal meninigitis • Second most common meningitis • pneumococcus, most common • Fatal if untreated • Responds well to antibiotic therapy • penicillin • Also causes fulminant Meningococcemia
Fulminant meningococcal septicaemia presents with: • Extensive haemorrhage into the skin • Hypotension • Shock • Confusion • Coma • DIC • Death (within a few hours of the onset of symptoms) • If adrenals are involved it is called as -Waterhouse-Friderichsen Syndrome (WFS)
Laboratory Diagnosis • Spinal fluid • Gram negative diplococci • within polymorphonuclear cells • Meningococcal antigens by CIEP • Culture • Blood agar, Chocolate agar
Virulence factor -Capsule • Capsule • inhibit phagocytosis • Anti-capsular antibodies • stop infection • Antigenic variation • sero-groups • Vaccine • multiple sero-groups