Download
1 / 26
260 likes | 622 Vues
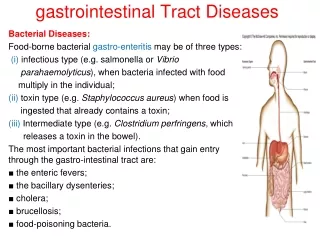
DISEASES OF THE GASTROINTESTINAL TRACT. Anatomy of stomach and duodenum. factors contribute to the protection of the gastric mucosa, including an impermeable epithelial cell surface covering, mechanisms for the selective transport of hydrogen and bicarbonate ions

E N D
factors contribute to the protection of the gastric mucosa, • including an • impermeable epithelial cell surface covering, • mechanisms for the selective transport of hydrogen • and bicarbonate ions • the characteristics of gastric • mucus. • These mechanisms are collectively referred to as • the gastric mucosal barrier.
GASTRITIS: Inflammation of the gastric mucosa • ACUTE GASTRITIS: • Aetiology: 1. Excessive use of non-steroidal anti-inflammatory drugs 2. Cytotoxic drugs • 3. Excessive alcohol consumption 4. Spicy food 5. Excessive smoking 6. Systemic infections as salmonellosis 7. Stress conditions • CHRONIC GASTRITIS: • Aetiology and Pathogenesis: • 1. Chronic infection with Helicobacter pylori: Bacterial urease enzyme generates ammonia, this protects these bacteria from HCl and simultaneously has a toxic effect on gastric mucosa. • 2. Autoimmune gastritis due to formation of antibodies causing atrophy of acid secreting cells resulting in hypoacidity and anaemia. • 3. Toxic effects of excess alcohol and tobacco.
ACUTE ULCERS OF STOMACH AND DUODENUM • Acute ulcers are stress ulcers due to increased HCl and pepsin secretion. They are seen in cases of acute gastritis due to drugs, infection, steroid therapy and severe burns. • The ulcers heal with minimal fibrosis on removal of the cause.
Etiology of PUD Normal Increased Attack Hyperacidity Weak defense Helicobacter pylori* Stress, drugs, smoking
CHRONIC PEPTIC ULCERS • It is a defect within the mucosa of any portion of GIT exposed to acid-pepsin secretion. • Duodenal and gastric ulcers are the commonest with male to female ratio of 3 to 1. • Gastric ulcers are usually single. Duodenal ulcers are commonly multiple. • Aetiology: • Predisposing factors: Excessive use of non-steroidal anti-inflammatory drugs, steroid drugs, excessive alcohol consumption, spicy food, excessive smoking and mental stress.
Pathogenesis of duodenal ulcer: • Hereditary predisposition: The disease has a familial tendency. It is more commonly observed in blood group O persons. • Hyperacidity • Infection by H. pylori • Pathogenesis of gastric ulcer: • Gastric ulcers have no genetic predisposition. Hyperacidity is not the cause of the disease. • The possible cause of gastric ulcer is mucosal devitalization by H. pylori (by enzymatic effect of the bacteria and not by hyperacidity) or by localized mucosal ischaemia. • Complications: • Haemorrhage, perforation. • Malignant change occurs in 1% of gastric ulcers.
Infective gastritis. H. pylori appears on silver staining as small, curved rods on the surface of the gastric mucosa. Gastric ulcer. The stomach has been opened to reveal a sharply demarcated, deep peptic ulcer .
Immune System Disorders Four Types of Hypersensitivity Reactions: Type I (Anaphylactic) Reactions Type II (Cytotoxic) Reactions Type III (Immune Complex) Reactions Type IV (Cell-Mediated) Reactions
Type I (Anaphylactic) Reactions Occur within minutes of exposure to antigen Antigens combine with IgE antibodies IgE binds to mast cells and basophils, causing them to undergo degranulation and release several mediators Anaphylactic shock, bronchial asthma, hay fever Anaphylactic shock: vascular dilatation, massive drop in blood pressure, mucus production. Can be fatal in minutes.
Type II (Cytotoxic) Reactions Involve phagocytosis or activation of complement by IgG or IgM binding to an antigenic cell. Antigenic cell is lysed. Ex: autoimmune hemolytic anemia Some Blood transfusion reactions: Rh Blood incompatibility:
Type III (Immune Complex) Reactions Involve reactions against soluble antigens circulating in serum. Usually involve IgA, IgG or IgMantibodies. Antibody-Antigen immune complexes are deposited in organs, activate complement, and cause inflammatory damage. Glomerulonephritis: Inflammatory kidney damage.
Type IV (Cell-Mediated) Reactions Involve reactions by Tcells. First contact sensitizes person. Subsequent contacts elicit a reaction. Reactions are delayed by one or more days (delayed type hypersensitivity). Delay is due to migration of macrophages and T cells to site of foreign antigens. Tuberculosis Contact dermatitis
Autoimmune Diseases Loss of self-tolerance leads to production of antibodies or T cells that react against one’s own antigens. Immune system response to self antigens causes damage to organs. Types of autoimmune disorders: Cytotoxic (Type II reactions) Immune complex (Type III reactions) Cell-mediated (Type IV reactions)
Autoimmune Diseases A. Type II (Cytotoxic) Autoimmune Reactions Involve antibody reactions to cell surface molecules, without cytotoxic destruction of cells. Grave’s Disease: Antibodies attach to receptors on thyroid gland and stimulate production of thyroid hormone. Symptoms: Goiter (enlarged thyroid) and bulging eyes. Myasthenia gravis: Progressive muscle weakness. Antibodies block acetylcholine receptors at neuromuscular synapse.
Autoimmune Diseases B. Type III (Immune Complex) Autoimmune Reactions Systemic Lupus Erythematosus (collagen disease): . Autoantibodies are formed,immune complexesform deposit under skin, joints, in kidneys, blood vessels, and central nervous system. Inflammation interferes with normal function of these sites (arthritis, rash, kidney damage). Most patients die from kidney damage.
Autoimmune Diseases B. Type III (Immune Complex) Autoimmune Reactions (Continued) Rheumatoid Arthritis (collagen disease): IgM or IgGautoantibodies (rheumatoid factors) against IgG form complexes in joint, leading to inflammation and cartilage damage. Often causes finger and joint deformities.
COLLAGEN DISEASES (connective tissue diseases): • Definition: Group of autoimmune diseases characterized by the same type of injury to collagen in different tissues • Ex: Rheumatic fever, rheumatoid arthritis, systemic lupuuserythrematosis, Scleroderma, Dermatomyositis
Autoimmune Diseases Type IV (Cell-Mediated) Autoimmune Reactions (Continued) Insulin-dependent (Type I or Juvenile) Diabetes Mellitus: . Characterized by insufficient insulin production due to immunological destruction of insulin-secreting cells of the pancreas by T cells. Usually develops before the age of 15. Treated with insulin injections.