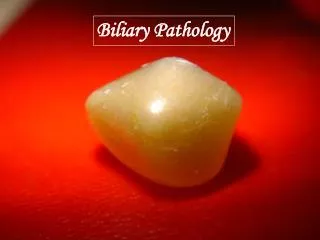
Biliary System
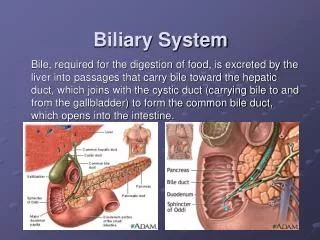
Biliary System. Bile, required for the digestion of food, is excreted by the liver into passages that carry bile toward the hepatic duct, which joins with the cystic duct (carrying bile to and from the gallbladder) to form the common bile duct, which opens into the intestine. Gallbladder.

Biliary System
E N D
Presentation Transcript
Biliary System Bile, required for the digestion of food, is excreted by the liver into passages that carry bile toward the hepatic duct, which joins with the cystic duct (carrying bile to and from the gallbladder) to form the common bile duct, which opens into the intestine.
Gallbladder • The gallbladder functions as a resevoir for bile produced by the liver. It is 7-10cm long, 3cm wide at its broadest measure, and has a capacity of 30-50ml. • The gallbladder is divided into 3regions : fundus, body, and neck.
Bile produced by the left and right portions of the liver travel through the right and left hepatic ducts (1-2mm in diameter). These two ducts join to form the common hepatic duct. • The union of the common hepatic duct and cystic duct forms the common bile duct (up to 6mm in diameter. Diameter increase 0.5-1mm per decade). • The common bile duct passes posterior to the first portion of the duodenum. It then descends via a groove on the superolateral portion of the posterior head of the pancreas, sometimes traveling through the pancreas head. • At the head of the pancreas, the common bile duct meets the pancreatic duct, and they exit into the second part of the duodenum, forming the hepatopancreatic ampulla (or ampulla of Vater).
Indirect Imaging: Indirect imaging involves non-invasive radiologic techniques including: US, plain film, CT, (MRCP) Oral ,IV Cholecystography Nuclear IDA scan (Cholescintigraphy) Direct Imaging: involves invasive radiologic procedures, which include: ERCP Operative and T-tube cholangiogram PTC (Imaging Modalities)
Plain Radiography • To detect either stones, calcification or gas in the biliary system.
Emphysematous cholecystitis Porcelain GB
Ultrasound • Is the first and the most commonly obtained method of examination in patients with RUQ pains, abnormal LFTs, or suspected liver masses. • Is a noninvasive and excellent screening tool. • Used to evaluate the presence of bile duct obstruction and gallstones as well as to distinguish a solid lesion from a cystic one. • The patient should be NPO (nothing-by-mouth) for imaging the biliary tract with ultrasound. Fasting distends the gallbladder and bile ducts and reduces bowel gas that may obscure visualization of portions of the gallbladder. Food may increase the thickness of the gallbladder wall imitating pathological wall thickening. Four hours is sufficient fasting for small children, and 6-8 hours for age 12 to adult. They should be told not to smoke during the fasting period since smoking causes the bile ducts to contract.
Technique of exam • Begin the exam with the patient in the supine position . The patient can be moved to the left posterior oblique ,left decubitus or even upright position.
Obtain full length of gallbladder from the portal vein to fundus (7-10cm) and transverse images (3cm) at representative levels. Measure GB wall thickness (up to 3mm) perpendicular to wall.Document any stones or biliary dilatation.
If stones are seen, evaluate if they are mobile or impacted. Move the patient into upright or lateral decubitus positions to demonstrate stone mobility. Rolling stone sign - movement of gallstones with GB with position change Note the change of position of the stones from (near the neck of GB )to its fundus when he changed his position from supine to decubitus position
Obtain full length of common bile duct (CBD) or as much as possible, and measure CBD diameter(N up to 6mm till the age of 60 then it increases 1mm each year).
Acquire longitudinal and transverse views of pancreatic head.
Endoscopic Ultrasonography • EUS uses ultrasound probes carried on endoscopes, so that ultrasound images can be obtained from inside the gastrointestinal tract. • Using ultrasound imaging from inside the body helps prevent the artifacts that can occur when imaging through the abdominal and chest wall. Degradation of the image by bone, fat, and bowel gas can be avoided. In addition, higher frequencies of ultrasound can be used. The higher the frequency the shorter the penetration depth, but because EUS places the ultrasound probe by endoscopy very close to the area to be examined, the smaller imaging area is not a problem
Note the stone(red arrow)causing strong acoustic shadowing (yellow arrow) is seen within the dilated CBD Note the stone within the dilated CBD
Computed Tomography (CT) • While CT is not the imaging modality of choice for visualizing the biliary tree directly it is useful in diagnosing liver, gallbladder, and pancreatic disease. • CT can identify pathological dilation of the intra&extrahepatic bile ducts it also can help in identification of the cause of obstruction as it can detect pancreatic cancer with 100% accuracy , The sensitivity for identifying bile duct stones is low; however, in a few cases a stone in the bile ducts can be identified. • CT also can identify gallstones, cholecystitis &GB cancer
Note the dilatation of the biliary radicals at the first image ,can you identify the cause at the second image (cancer head of pancreas) Common bile duct stone & GB stones
Spiral CT cholangiography • 3-D CTC as a non-invasive and sensitive technique for the diagnosis of biliary diseases with high diagnostic accuracy will greatly increase the detection rate of biliary diseases.
Technique of CT cholangiography • One hundred milliliters of cholangiographic contrast material iotroxate meglumine (Biliscopin) is infused IV over a period of 30 min, and helical CT cholangiography was performed 30 min later. After rolling the patient to mix bile and contrast material in the gallbladder • Multi-slice helical CT, using scanning mode HQ, 120 kV, 270-280 mA, 0.8 s/r, pitch 3, with table incrementation rate of 11.25 mm/s. The scope of scanning covered the whole biliary tree. 5 mm in thickness at 5 mm intervals was used, followed by an overlapping reconstruction of 3.75 mm in thickness at 2.0 mm intervals, or 3.75 mm in thickness at 3.75 mm intervals, followed by an overlapping reconstruction of 2.5 mm in thickness at 1.0 mm intervals. Among the three-phase enhancement scanning, the portal phase was selected for a reconstruction of 3.75 mm in thickness at 2.0 mm intervals. • All imaging data were sent to the workstation .Based on actual requirements, maximum density projection (MIP), minimum density projection (MinP), surface shaded display (SDD), CT virtual endoscopy (CTVE)
Magnetic resonance cholangiopancreatography (MRCP) • MRCP is a non-invasive technique that delineates the pancreatic and biliary ductal systems, while providing projectional and cross sectional images of the ducts. MRCP does not require administration of IV contrast material; it is based on T2-weighted images, which depict static fluid (including bile and pancreatic secretions), with a higher signal intensity. MRCP also avoids the invasive complications of ERCP. With the recent improvements in MRCP, it is superceding ERCP for many of its diagnostic indications. MRCP is inferior to ERCP in several respects however. The spatial resolution of MRCP is lower than that of ERCP. Furthermore, ascites or fluid collections in the upper abdomen can interfere with the visualization of the pancreatic and biliary ducts.
Technique of MRCP • MRCP images are taken in axial, coronal, and 3-D formats providing imaging referencing in multiple planes. It is important that the entire gallbladder, biliary ducts, and pancreas are included in the axial, coronal, and 3-D images. Two techniques are combined for imaging the biliary tract: multisection thin-slice and single-slice thick-slab MRCP. Studies show that these techniques should be combined in the imaging protocol to get the most out of the unenhanced and enhanced MR scan. Intravenously administered fentanyl before MRCP has been shown to improve the qualitative and quantitative visualization of the biliary tree. The reason for both techniques is that single-shot thin-slice imaging is superior to multisection thin slice for bile duct imaging.
Oral Cholecystography • The oral cholecystogram (OCG) is a purely historical examination that studied the opacification of the gallbladder. This study was once the diagnostic standard for imaging the gallbladder before ultrasound and CT reached the current level of image quality. The basic process involved the patient not eating any fatty foods, or being N.P.O (nothing by mouth) about 6 hours before ingesting oral contrast media. This was in the form of tablets (brand name-Telopaque), that when dissolved the media is absorbed into liver and secreted in bile
Nuclear IDA scan (Cholescintigraphy) • It uses the radioisotope imino diacetic acid (IDA) to image part of the biliary system. In the past the IDA scan has been called the HIDA scan. The most common reason for physicians requesting this scan is to evaluate the: 1-functioning of the cystic duct in case of suspected cholecystitis 2-can also detect biliary obstruction, 3- bile leak, 4- Atresia. • The IDA scan is a dynamic scan that assesses function of the gallbladder and cystic duct patency. Technetium-99m-IDA agents such as Choletec or Hepatolite are administered intravenously. These agents are bilirubin analogues having the same biliary uptake as bilirubin used to make bile, but are not conjugated to bilirubin. Then they are secreted into the biliary tract allowing them to be taken up by the liver and secreted into the biliary tract and concentrated in the normal functioning gallbladder. When the biliary tract is functioning properly the entire bilirubin pathway from filling of the gallbladder to passage into the common bile duct and duodenum should be visualized.
Endoscopic Retrograde Cholangiopancreatography (ERCP) • ERCP is a combined endoscopic and radiographic procedure that images the biliary and pancreatic ducts. ERCP is performed with a side-viewing duodenoscope which has an instrumentation channel that allows for the insertion of the cannulation catheter into the major or minor duodenal papilla. A water-soluble contrast agent (60 % iodine) is injected into the ductal system using fluoroscopy for imaging. It is important to obtain adequate ductal filling without over-distending the system. (During interventional procedures, a guide-wire can be inserted through the cannulation catheter, for subsequent insertion of additional instruments like papillotomes, drainage devices, cytology brush, etc.) Althought ERCP is an important diagnostic tool in the evaluation of patients with suspected biliary and pancreatic disorders, MRCP is superceding ERCP for some of its indications.
ERCP Indications • >Biliary disease--Jaundice--Cholestasis--Cholangitis--Choledocholithiasis/gallstones--Tumors--Primary biliary sclerosis>Pancreatic Disease--Acute gallstone pancreatitis--Recurrent acute pancreatitis--Chronic pancreatitis--Pancreatic pseudocyst, abcess--Pancreatic tumors>Pre- and/or post-op duct eval>Evaluation post liver transplant>Sphincter of Oddi manometry>Unexplained upper abdominal pain>Therapeutic interventions--Biopsy/cytology--Sphincterotomy--Stone extraction--Lithotripsy--Stent placement--Balloon dilation of strictures--Pseudocyst drainage--Irradiation
Complication Pancreatitis Cholangitis Infection Perforation Significant bleeding Mechanism/comment Secondary to over-distention of pancreatic ducts with contrast extravisation into parenhymal tissue, Antibiotics are initiated if biliary obstruction is present and cannot be relieved. Most common organisms include GNR (E. coli, Klebsiella) Bacteremia, pseudocyst, and abcess formation Sphincterotomy, ampulla in duodenal diverticulum Sphincterotomy ERCP complications
PostOperative Cholangiography (T-tube Cholangiogram) • Postoperative t-tube cholangiography is performed to exclude a retained bile duct calculus or to assess for any surgical complications such as a bile duct leak before removal of the t-tube. The study is usually performed 7-10 days after surgery.
Percutaneous Transhepatic Cholangiography (PTC) • This is another radiographic study that is purely historical and is not done in modern radiographic imaging. It was both a diagnostic procedure in cases of suspected obstructive jaundice, and therapeuticin that dilated bile ducts could be drained during the procedure. Occasionally a stone could be removed by this procedure eliminating the risk of open surgical intervention. Today there are many other invasive procedures with lower risk than PTC. This study was a type of invasive cholangiography that involved direct puncture of the biliary ducts. A fine needle was passed from the skin surface through the liver into a biliary duct. Risk of the procedure included possible puncture of the lung, bleeding from the liver and vascular injury. This was not an easy procedure to perform so benefit of the procedure had to far outweigh its risk before it was performed.
Developmental anomalies&Normal variants • Gallbladder ectopia. Intrahepatic gallbladder (GB) demonstrated on CT scan
Gallbladder ectopia. Situs inversus with left-sided gallbladder