Download
1 / 19
190 likes | 287 Vues
With meeting discussion notes. To join the meeting: Phone Number : +1 770-657-9270 Participant Passcode : 943377#. Care Plan (CP) Meeting - Minutes October 31, 2012 1700-1830 EDT. Laura Heermann Langford (Laura.Heermann@imail.org) Stephen Chu (stephen.chu@nehta.gov.au)

E N D
With meeting discussion notes To join the meeting: Phone Number: +1 770-657-9270Participant Passcode: 943377# Care Plan (CP) Meeting -Minutes October 31, 20121700-1830 EDT Laura Heermann Langford (Laura.Heermann@imail.org) Stephen Chu (stephen.chu@nehta.gov.au) *Care Plan wiki:http://wiki.hl7.org/index.php?title=Care_Plan_Initiative_project_2011 HL7 Patient Care Work Group
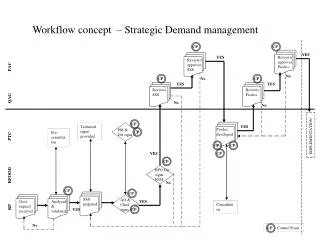
Tentative: October 31, 2012 (subject to change) • Modelling update • Clarifying “master care plan”/”care coordination plan” – definitions • Master care plan – domain specific detail care plan relationship (Plan-plan compositions, that is, peer-peer or hierarchical connections between CPs and/or between CP and POC) • Inter-detail care plan relationship – inbound and outbound risk • Care plan concepts – terminology and definitions
Modeling • Enrique Meneses
Discussion Notes • Have worked on classes in EA extracted from the Storyboards • Needs more work before reviews. • Enrique and Jon will continue working in pairs offline. Jon could work on it and propose reviewing in this larger group in 2 weeks (next meeting) • Jon has also begun modeling a class diagram in EA describing relations and how they would integrate into the model currently in progress. • Enrique will work to set up a shared model repository for Jon to have easier access to the model. • Underlying files for the repository would be password protected. • Need the corporate version EA to access.
Care Plan Relationships (linked or nested…master VS Coordinated) • Jon/Laura/Stephen…
Discussion Notes • Have come to agreement there is an all over coordinating care plan… the Master Patient Care Plan. • Agreements • The master care plan is the specialty care plans interleaved. The service could be created to accommodate the reconciliation • The concept of the patient or someone else being able to “hide” or “conceal” data from one care giver or provider or another exists – but will be addressed later. • Examples of content that would need reconciliation--Meds, problems, history, allergies, advanced directives, • Discussions…. • Care plan might inform the plan of care, • Plan of care = episodic plan • Master care plan and specialty care plan – both could inform the plan of care… • This is all very difficult to follow would be helpful to have a diagram. Perhaps – use a problem specific….such as hypertension, or use one of the use cases we have developed – use the chronic care storyboard ….Laura to present next time… • Terminology – to refer to Master Plan and the Specialty Plan that are really detailed but likewise relatively long term. • History of the plan and reports of activities from the plan are part of the medical record. • In the case of some observations – you may have the meta data on the care plan (blood pressure stead) instead of the last 14 readings… • Active goals stay on the care plan, resolved/completed goals become part of the medical record • Some goals, or medical issues may stay on the care plan even if they are complete or resolved…because they are relevant to the overall care. Such as “smoked 4ppd for 30 years until last month…..” • Questions- • How much detail should be in the master care plan
Discussion Notes • Jon has taken extensive notes Laura to send her notes to him for consolidation. • 5 November 2012 update: See next slides for consolidated minutes
Discussion Notes Defining the master CP Have come to agreement there is an overall coordinating care plan… the Master Patient Care Plan. Example domain-specific CPs: Dental hygienist, Cardiologist The master care plan is the specialty care plans interleaved. The service could be created to accommodate the reconciliation Master is high level coordinating care plan, shared among interdisciplinary providers that are specific to problem topic or domain of practice. A Coordination engine coordinates them. Specialty plans don’t have to physically collected submitted to central storage, but can be federated , A CSS service, when queried for the MCP of a particular patient, could deliver not only its local common root content, but it could also follow pointers to the CSS interfaces of the specialty plans. Thus the MCP becomes virtually centralized for all its clients. This is fully analogous to the full-continuum patient record, but it’s for the plans. Agreed in principal. What Terminology to use? to refer to Master Plan and the Specialty Plan that are really detailed but likewise relatively long term. Master Plan will include its own content in addition to the specialty content, such as the Blood Glucose goals for a DM patient. Subsetting Views The concept of the patient or someone else being able to “hide” or “conceal” data from one care giver or provider or another exists – but will be addressed later. Some elements only reside in master – like medication list. Also advance directives Examples of content that would need reconciliation--Meds, problems, history, allergies, advanced directives, Relevant fragments will be created among disjoint plans but can be reconciled into the MCP Master is always inclusive of specialties., but user can filter views. The CP subject matter scope is one thing (e.g. whether to include all or some specialties or a single specialty). Then there could be different ways to sort it or present it – such as nested-plans, versus interleaved plan parts. Discussions….
Discussion Notes Relationships of CP vs. POC Care plan might inform the plan of care, Plan of care = episodic plan Master care plan and specialty care plan – both could inform the plan of care… Then the POCs can update the master goals and progress, outcomes and recommendations, and procedural problems for ongoing management. Laura will prepare a graphic to illustrate. SC: Perhaps – use a problem specific….such as hypertension, or use one of the use cases we have developed – use the chronic care storyboard. MD or COPD, walk through to create diagram. Keeping the MCP Lean History of the plan and reports of activities from the plan are part of the medical record. Optometry every 6 months – goes into master. But … patient deteriorated. Laser treatment. Cataract has detailed cp to manage it. MCP does not need to know those details. MCP neds to know the visit times, that appointments were made. Procedure operation occurred, summary gets into the plan. The “record” is not part fo the care plan. Anything that the opthalmologist considers “plan” should be considered part of the care plan. When the two weeks pass, its part of the record, not the plan. Some believe that relevant history must be retained to provide context. If goal is to stop smoking, is your goal to stop or to not smoke. The history helps to manage the risk. So an observation can be designated for retention in plan. In the case of some observations – you may have the meta data on the care plan (blood pressure steady) instead of the last 14 readings… We need the goal and the outcome. Then from outcome might have meta observation – the observation about the observation. Like 14 BPs daily over 7 days. These make a trend – a meta observation like “stabilized” Perhaps this is the key to preventing the whole record from getting sucked into the CP. CP audit trail would show effective-dated view of the Plan. Goal of eye operation is to restore vision and …. No infection. No breakdown of cornea around incision. Strategy to ensure that goals are achieved. Active goals stay on the care plan, resolved/completed goals become part of the medical record The MCP is prospective, so some content goes obsolete as time passes.
Discussion Notes Active Guides future decisions Some goals, or medical issues may stay on the care plan even if they are complete or resolved…because they are relevant to the overall care. Such as “smoked 4ppd for 30 years until last month…..” JF comment while editing: Meta-observations could be stored indefinitely (according to local policy or preference), but merely filtered out by time window option for retrievals. We may need to the ability to designate some items as permanent (perhaps there are a small number of alternative “expiration policies” that a user could put on content) Questions- How much detail should be in the master care plan Assessments Assessment is a process that is not part of the plan, but a process where the plan and the record come together. Assessment is where you compare the status (which is in the record) to the goal (care plan). The info is met-goal. That goal then stays on the plan? Some goals for chronic will be retained. Goal will then be to “maintain” BP at 120. Milestone goals, Maintenance Goals there will be long term (permanent) and short term goals. Return to full ambulation after surgery is a short term goals. BP control is form now on. SC: might state long term goal as normotensive. Milestone goals are incremental or interim toward maintenance goal. The goal issue is not unlike the problem list issue – resolved or inactive. There are also wellness goals that are not equivalent to controlling BP. Then there are personal goals that you set for yourself that may not fit into our previous categories of goals, e.g. healthy eating or periodic screening goals (colonoscopy every five yrs); personal goals like I want to dance at my daughter wedding.
Next steps • Next meeting • Continue discussion on the care plan relationships, what is included and not, definitions and terminology • Laura to have diagram ready to generate and refine further discussion • Drill down to goals at some point in the diagram to demonstrate how goals are added, updated, moved to medical record etc. • Laura to bring goal work to next meeting • Review modeling work as it is ready and needing discussion.
Inbound/Outbound Risks • Jon?…
Discussion Notes • Not yet addressed. Would like to get more of the previous discussion completed before addressing the inbound/outbound risks
Discussion Notes • Not addressed specifically on the call today. • Will be part of the continued discussion with the diagram next meeting
Next Agenda Future Meetings • Conference calls between now and January 2013 – see wiki 90 min., Wednesday 5-6:30pm US Eastern, fortnightly (every 2 weeks) Starting September 19
Next meeting Agenda- November 14 (Lead: Laura) Upcoming Topics • . • Future topic