Download
1 / 65
760 likes | 1.85k Vues
Shoulder Examination & Common Pathology. Mr David Rose FRCS Consultant Shoulder & Elbow Surgeon. My Background. Medical School: Royal Free (University of London - 2000) South West Thames Ortho Rotation (St Georges) Fellowships:

E N D
Shoulder Examination & Common Pathology Mr David Rose FRCS Consultant Shoulder & Elbow Surgeon
My Background • Medical School: Royal Free (University of London - 2000) • South West Thames Ortho Rotation (St Georges) • Fellowships: • Johns Hopkins, USA 2008/09 (Research – Shoulder/Upper Limb) • Perth Orthopaedic & Sports Medicine Centre, Perth, Australia 2012/13 (Sports Medicine Surgery) • Addenbrooke’s, Cambridge 2013/14 (Shoulder & Elbow Surgery)
Current Position • Consultant Orthopaedic Surgeon Maidstone & Tunbridge Wells NHS Trust • Started February 2014 • Main Interests: Arthroscopic and Reconstructive Surgery of the Shoulder & Elbow
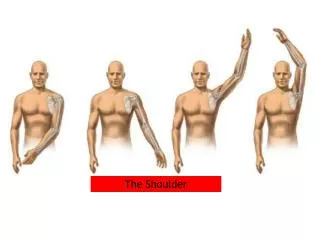
Look Feel Move Special Tests COMPARE SIDES Examination
Cervical Spine Thoracic Spine Neck Examination Cardiac Disease Referred Pain
Muscles - wasting, winging Deformity - malunion, scars, ACjt Look
Scapular Wasting Look
Winging Look
Compare sides (great variation) Passive v Active Loss of Motion - Mechanical - Muscular - Pain Inhibition - Neurological Range of Motion
Rotator Cuff Disease Instability Special Tests
Muscle Strength Impingement ACjt Pathology Biceps Pathology Rotator Cuff Disease
Jobe’s Supraspinatus
Gerber’s Subscapularis
Napolean Subscapularis
Neer’s Impingement
Hawkin’s Impingement
Scarf AC Joint
Speed’s Biceps
Yergason’s Biceps
Generalised Joint Laxity Anterior Instability Posterior Instability (no apprehension) Labral Pathology Instability
Sulcus Sign Instability
Apprehension Instability
Relocation Test Instability
Jerk Test Posterior Instability
O’Brien’s Labrum
Instability Rotator Cuff Disease Frozen Shoulder OA / RhA Shoulder Pathology
Young - Instability Middle-Age- Rotator-Cuff & Frozen Shoulder Elderly- Rotator-Cuff & OA Common Shoulder Pathology
Instability Rotator Cuff Disease Frozen Shoulder OA / RhA Shoulder Pathology
Instability Traumatic v Atraumatic Bankart Tear Labral Tear Capsular Laxity
Muscle Patterning Problems Teenage Female Uni- or Bi-lateral Physiotherapy (specialist) Generalised Joint Laxity
Management Reduction Sling immobilisation until comfortable Physiotherapy Recurrence ↓ with ↑ age ? Rotator cuff tear > 50yrs First Time Dislocator
Management Activity modification Surgical Stabilisation – (open / arthroscopic / bony) Recovery - 2 - 3 wks - immobilisation - 4 - 6 wks - day to day activities - 4 - 6 mths - contact sports Outcome 90 – 95 % stable at 2 years Recurrent Anterior Dislocation
Instability Rotator Cuff Disease Frozen Shoulder OA / RhA Shoulder Pathology
Spectrum tendonitis ↓ partial tear ↓ full thickness tear ↓ cuff arthropathy Rotator Cuff Disease Tendinosis Tear
Incidence of Rotator Cuff Defects Arthrogram Study (asympt) 60+yrs 50% 80+yrs 80% MRI Study (asymptomatic) 19-39yrs 2% PT RCT 40-60yrs 28% RCT Rotator Cuff Disease
Treat the Symptoms Non-Operative (+ activity modification) Operative Rotator Cuff Disease
“Orthotherapy” - 3 Phases Control the Pain- NSAID - Cortisone Injection Regain ROM - Physio / exercises Muscle Strengthening- Physio / exercises - Activity modification Management - non-operative
Steroid injection • I prefer posterior approach • 70-80% accuracy when performed “blind” • 40mg depomedrone; 5-10mls marcaine 0.25%
Indications for Surgery Failure or relapse following adequate non-operative treatment (6mths +) Management - operative
Expectations from Surgery Pain relief Variable functional recovery NOT a new shoulder –‘degenerate tissue’ Management - operative
Address the Pathology Arthroscopic Subacromial Decompression AC joint Excision Rotator Cuff Repair Arthroplasty Muscle Transfer Management - operative
Double-Row Repair Rotator Cuff Repair Double-row arthroscopic rotator cuff repair: Re-establishing the footprint of the rotator cuff. Lo IKY et al. Arthroscopy 2003
Management – (failed non-operative / ACUTE event) arthroscopic decompression +/- rotator cuff repair Recovery ASD - immediate mobilisation - 3 – 6 months optimal recovery Cuff Repair - 1 – 3 weeks sling - 3 – 6 months optimal recovery Outcome 85% full recovery, 10% significantly better, 5% no worse! Rotator Cuff Disease