Download
1 / 20
200 likes | 399 Vues
4 YEARS SURVIVAL OF 100 HCC PATIENTS TREATED WITH DC BEAD: A RETROSPECTIVE ANALYSIS . Marta Burrel Vascular Interventional Unit Barcelona Clinic Liver Cancer Group Hospital Clínic. Barcelona, Spain. Normal. BCLC Classification and Treatment Schedule. HCC. Stage D. Stage 0.

E N D
4 YEARS SURVIVAL OF 100 HCC PATIENTS TREATED WITH DC BEAD: A RETROSPECTIVE ANALYSIS Marta Burrel Vascular Interventional Unit Barcelona Clinic Liver Cancer Group Hospital Clínic. Barcelona, Spain.
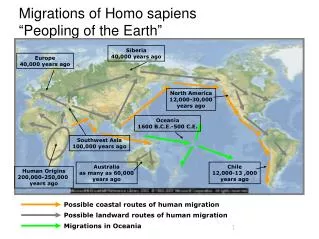
Normal BCLC Classification and Treatment Schedule HCC Stage D Stage 0 Stage A-C PST 0, Child-Pugh A Okuda 1-2, PST 0-2, Child-Pugh A-B Okuda 3, PST >2, Child-Pugh C Very early stage (0) Single< 2cm. Carcinoma in situ Early stage ( A) Single or 3 nodules < 3cm, PS 0 Terminal stage (D) Advanced stage (C) Portal invasion, N1,M1, PS 1-2 Intermediate stage ( B) Multinodular, PS 0 Single 3 nodules <3cm Portal pressure/ bilirubin Associated diseases Increased No Yes Liver Transplantation (CLT / LDLT) PEI/RF TACE Sorafenib Resection RCT: 40% - 50% at 3 yr vs 10% at 3yr Symptomatic treatment Curative Treatments: 50% - 75% at 5 years Forner et al. Semin Liver Dis. 2010 Feb;30(1):61-744
Lipiodol TACE improves survival in a selected group of HCC patients Survival probability TACE Control 1 year 57% 32% 2 years 31% 11% Survival probability TACE Control 1 year 82% 63% 2 years 63% 27% 35% objective response > 6 months Independent prognostic factor Lo et al. Hepatology 200235(5):1164-71 Llovet et al. Lancet 200218;359(9319):1734-9
Systematic Review of RCT for Unresectable HCC • Random effects model (DerSimonian & Laird) OR (95% CI) 0.5 0.01 0.1 10 100 1 2 Author,Journal, year Cumulative (pts) Lin, Gastroenterology 1988 63 GETCH, NEJM 1995 159 Bruix , Hepatology 1998 239 Pelletier, J Hepatol 1998 312 Lo, Hepatology 2002 391 Llovet, Lancet 2002 503 2p=0.086 OVERALL 503 2p=0.017 Heterogeneity: Q:7.73P=0.14 Median survival : ~ 20 months Favors treatment Favors control Llovet and Bruix. Hepatology 2002
Cohort studies with TACE-DC Beads . Improved Objective Response . Better tolerance
Randomization N=87 Chemoembolization vs Bland Embolization Compensate cirrhosis Child-Pugh A –B ECOG o-1 Number of nodules No difference in both groups Bland Embolization (n=41) TACE with DCB (n=43) • TACE-DEB better than Bland Embolization • Local response. Overall Response (p=0.04) • Fewer recurrence. At 9 months (p=0.002) • Longer TTP (p=0.008) Malagari et al.Cardiovasc Intervent Radiol. 2010 Jun;33(3):541-51. Epub 2009 Nov 24.
TACE - DC Beads: Randomised Studies Precision V End Point: Negative Doxorubicin-Related Side Effects: Lammer et al. Cardiovasc Intervent Radiol (2010), 33(1):41-52
SURVIVAL DATA AFTER TACE IN PATIENTS WITH HEPATOCELLULAR CARCINOMA (HCC) IN 2010: IMPACT ON CLINICAL PRACTICE AND RESEARCH
OBJECTIVES • Evaluate the survival of HCC patients treated with TACE-DEB following a strict selection (preserved liver function, absence of cancer related symptoms, extrahepatic spread or vascular invasion) • Evaluate causes of untreatable progression (UTP)
PATIENTS AND METHOD • HCC patients treated by TACE-DEB between February 2004 and March 2010 • Retrospective review of: • baseline characteristics • development of treatment related adverse events • overall survival
RESULTS • - 97 patients evaluated • - Median follow up 24.4 months (2.6-79.6) • At the time of evaluation • 31 patients had died • 2 received transplantation • 22 had received Sorafenib because of progression not amenable for TACE
Función de supervivencia 1,0 Censurado 0,8 0,6 0,4 0,2 0,0 0,00 20,00 40,00 60,00 80,00 Survival (months) Results: Survival Median whole cohort survival : 47.7 months (95%CI: 36.6-58.8)
Results: Survival OS 54.2 months for stage A OS 40.2 months for stage B Survival after censoring follow-up at the time of transplant or Sorafenib 40.2 months for BCLC A 31.9 months for BCLC B
Evolutionary events after TACE The untreatable progression concept TACE Objective response No objective response Retreatment strategy 2nd-line option Progression Treatable (i.e. additional small HCC) Untreatable (i.e. vascular invasion, M1) or Liver failure/contraindication TACE HCC progression controlled Prof Bruix.Personal communication
Causes of untreatable progression leading to Sorafenib administration n= 22
Precision V: Potential patients with UTP J Lammer et al. Cardiovasc Intervent Radiol. 2010 Feb;33(1):41-52.
CONCLUSIONS • Current survival of non-ressectable HCC patients within stages A and B is 47,7 months • Current survival of BCLC B patients is 40,2 months • These new data update the previous survival results obtained from Lipiodol-TACE, which impacts in clinical practice and research purposes