
Behavioral and Clinical Risk Factors on HIV-Associated Dementia in Prisoners
This study examines the associations between behavioral and clinical factors and performance on neuropsychological screening tests for HIV-associated dementia (HAD) in an incarcerated population. The prevalence of HAD in the population is estimated, and the utility of screening tests for cognitive impairment in this population is assessed.

Behavioral and Clinical Risk Factors on HIV-Associated Dementia in Prisoners
E N D
Presentation Transcript
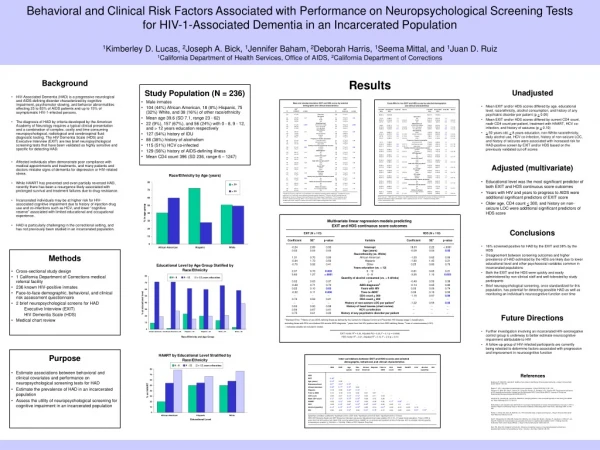
Behavioral and Clinical Risk Factors Associated with Performance on Neuropsychological Screening Tests for HIV-1-Associated Dementia in an Incarcerated Population1Kimberley D. Lucas, 2Joseph A. Bick, 1Jennifer Baham, 2Deborah Harris, 1Seema Mittal, and 1Juan D. Ruiz1California Department of Health Services, Office of AIDS, 2California Department of Corrections Results
Background • HIV-Associated Dementia (HAD) is a progressive neurological and AIDS-defining disorder characterized by cognitive impairment, psychomotor slowing, and behavior abnormalities affecting 25 to 65% of AIDS patients and up to 15% of asymptomatic HIV-1-infected persons. • The diagnosis of HAD by criteria developed by the American Academy of Neurology requires a typical clinical presentation and a combination of complex, costly and time consuming neuropsychological, radiological and cerebrospinal fluid diagnostic testing. The HIV Dementia Scale (HDS) and Executive Interview (EXIT) are two brief neuropsychological screening tests that have been validated as highly sensitive and specific for detecting HAD.
Affected individuals often demonstrate poor compliance with medical appointments and treatments, and many patients and doctors mistake signs of dementia for depression or HIV-related stress. • While HAART has prevented and even partially reversed HAD, recently there has been a resurgence likely associated with prolonged survival and treatment failures due to drug resistance. • Incarcerated individuals may be at higher risk for HIV-associated cognitive impairment due to history of injection drug use and co-infections such as HCV, and lower “cognitive reserve” associated with limited educational and occupational experience. • HAD is particularly challenging in the correctional setting, and has not previously been studied in an incarcerated population.
Methods • Cross-sectional study design • 1 California Department of Corrections medical referral facility • 236 known HIV-positive inmates • Face-to-face demographic, behavioral, and clinical risk assessment questionnaire • 2 brief neuropsychological screens for HAD Executive Interview (EXIT) HIV Dementia Scale (HDS) • Medical chart review
Purpose • Estimate associations between behavioral and clinical covariates and performance on neuropsychological screening tests for HAD • Estimate the prevalence of HAD in an incarcerated population • Assess the utility of neuropsychological screening for cognitive impairment in an incarcerated population
Study Population (N = 236) • Male inmates • 104 (44%) African American, 18 (8%) Hispanic, 75 (32%) White, and 38 (16%) of other race/ethnicity • Mean age 39.6 (SD 7.1, range 23 - 62) • 22 (9%), 157 (67%), and 56 (24%) with 0 - 8, 9 - 12, and > 12 years education respectively • 127 (54%) history of IDU • 88 (38%) history of alcoholism • 115 (51%) HCV co-infected • 129 (56%) history of AIDS-defining illness • Mean CD4 count 396 (SD 236, range 6 – 1247)
Unadjusted • Mean EXIT and/or HDS scores differed by age, educational level, race/ethnicity, alcohol consumption, and history of any psychiatric disorder per patient (p < 0.05) • Mean EXIT and/or HDS scores differed by current CD4 count, nadir CD4 count per patient, treatment with HAART, HCV co-infection, and history of seizures (p < 0.10) • > 50 years old, < 8 years education, non-White race/ethnicity, daily alcohol use, HCV co-infection, history of non-seizure LOC, and history of seizures were associated with increased risk for HAD-positive screen by EXIT and/or HDS based on the previously validated cut-off scores
Adjusted (multivariate) • Educational level was the most significant predictor of both EXIT and HDS continuous score outcomes • Years with HIV and years to progress to AIDS were additional significant predictors of EXIT score • Older age, CD4 count < 300, and history on non-seizure LOC were additional significant predictors of HDS score
Conclusions • 16% screened positive for HAD by the EXIT and 38% by the HDS • Disagreement between screening outcomes and higher prevalence of HAD estimated by the HDS are likely due to lower educational level and other psychosocial variables common in incarcerated populations • Both the EXIT and the HDS were quickly and easily administered by non-clinical staff and well-tolerated by study participants • Brief neuropsychological screening, once standardized for this population, has potential for detecting possible HAD as well as monitoring an individual’s neurocognitive function over time
Future Directions • Further investigation involving an incarcerated HIV-seronegative control group is underway to better estimate neurocognitive impairment attributable to HIV • A follow-up group of HIV-infected participants are currently being retested to determine factors associated with progression and improvement in neurocognitive function
References • Berghuis JP, Uldall KK, Lalonde B. Validity of two scales in identifying HIV-associated dementia. J Acquir Immune Defic Syndr 1999,21:134-140. • Eggers C. HIV-1 associated encephalopathy and myelopathy. J Neurol 2002,249:1132-1136. • Farinpour R, Miller EN, Satz P, Selnes OA, Cohen BA, Becker JT, Skolasky Jr RL, Visscher BR. Psychosocial risk factors of HIV morbidity and mortality: findings from the Multicenter AIDS Cohort Study (MACS). Journal of Clinical and Experimental Neuropsychology 2003,25(5):654-670. • Langford TD, Letendre SL, Larrea GL, Masliah E. Changing patterns in the neuropathogenesis of HIV during the HAART era. Brain Pathology 2003,13:195-210. • Nomenclature and research case definitions for neurologic manifestations of human immunodeficiency virus-type 1 (HIV-1) infection. Report of a Working Group of the American Academy of Neurology AIDS Task Force. Neurology 1991,41:778-785. • Power C, Selnes OA, Grim JA, McArthur JC. HIV Dementia Scale: a rapid screening test. J Acquir Immune Defic Syndr Hum Retrovirol 1995,8:273-278. • Satz P, Morgenstern H, Miller EN, Selnes OA, McArthur JC, Cohen BA, Wesch J, Becker JT, Jacobson L, D’Elia LF, van Gorp W, Visscher B. Low education as a possible risk factor for cognitive abnormalities in HIV-1: findings from the multicenter AIDS Cohort Study (MACS). J Acquir Immune Defic Syndr 1993,6:503-511. • Stern RA, Silva SG, Chaisson N, Evans DL. Influence of cognitive reserve on neuropsychological functioning in asymptomatic Human Immunodeficiency Virus-1 infection. Arch Neur 1996,53:148-153.





















