PANCREATIC FUNCTION TESTS
BIOCHEMISTRY

PANCREATIC FUNCTION TESTS
E N D
Presentation Transcript
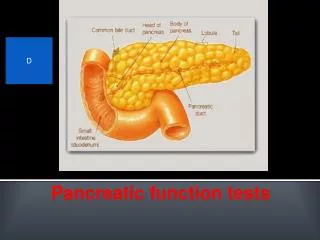
EXOCRINE PANCREAS : FUNCTIONS AND DISORDERS M.Prasad Naidu MSc Medical Biochemistry, Ph.D.Research Scholar
The pancreas secretes 1500–3000 mL of isosmotic alkaline (pH >8) fluid per day containing about 20 enzymes. • The pancreatic secretions provide the enzymes needed to effect the major digestive activity of the gastrointestinal tract and provide an optimal pH for the function of these enzymes.
Regulation of Pancreatic Secretion • The exocrine pancreas is influenced by intimately interacting hormonal and neural systems. • Gastric acid is the stimulus for the release of secretin from the duodenum, which stimulates the secretion of water and electrolytes from pancreatic ductal cells. • Release of cholecystokinin (CCK) from the duodenum and proximal jejunum is largely triggered by long-chain fatty acids, certain essential amino acids (tryptophan, phenylalanine, valine, methionine), and gastric acid itself. • CCK evokes an enzyme-rich secretion from acinar cells in the pancreas.
Water and Electrolyte Secretion • Bicarbonate is the ion of primary physiologic importance within pancreatic secretion. • The ductal cells secrete bicarbonate predominantly derived from plasma (93%) more than from intracellular metabolism (7%). • Bicarbonate enters through the sodium bicarbonate cotransporter with depolarization caused by chloride efflux through the cystic fibrosis transmembrane conductance regulator (CFTR). • Secretin and VIP, both of which increase intracellular cyclic AMP, act on the ductal cells opening the CFTR in promoting secretion. • CCK, acting as a neuromodulator, markedly potentiates the stimulatory effects of secretin. • Acetylcholine also plays an important role in ductal cell secretion. Bicarbonate helps neutralize gastric acid and creates the appropriate pH for the activity of pancreatic enzymes and bile salts.
Enzyme Secretion • The acinar cell is highly compartmentalized and is concerned with the secretion of pancreatic enzymes. • Proteins synthesized by the rough endoplasmic reticulum are processed in the Golgi and then targeted to the appropriate site. • Amylolytic enzymes such as amylase, hydrolyze starch to oligosaccharides and to the disaccharide maltose. • The lipolytic enzymes include lipase, phospholipase A2, and cholesterol esterase. Bile salts inhibit lipase in isolation, but colipase, another constituent of pancreatic secretion, binds to lipase and prevents this inhibition. Bile salts activate phospholipase A and cholesterol esterase.
Proteolytic enzymes include endopeptidases (trypsin, chymotrypsin), which act on internal peptide bonds of proteins and polypeptides; exopeptidases (carboxypeptidases, aminopeptidases), which act on the free carboxyl- and amino-terminal ends of peptides, respectively; and elastase. • The proteolytic enzymes are secreted as inactive precursors and packaged as zymogens. • Ribonucleases (deoxyribonucleases, ribonuclease) are also secreted. • Enterokinase, an enzyme found in the duodenal mucosa, cleaves the lysine-isoleucine bond of trypsinogen to form trypsin. • Trypsin then activates the other proteolytic zymogens and phospholipase A2 in a cascade phenomenon. • All pancreatic enzymes have pH optima in the alkaline range.
The nervous system initiates pancreatic enzyme secretion. • The stimulatory neurotransmitters are acetylcholine and gastrin-releasing peptides. • These neurotransmitters activate calcium-dependent second messenger systems, resulting in the release of zymogen granules.
Autoprotection of the Pancreas • Autodigestion of the pancreas is prevented by the packaging of pancreatic proteases in precursor form and by the synthesis of protease inhibitor [i.e., pancreatic secretorytrypsin inhibitor (PSTI) (SPINK1) ], which can bind and inactivate about 20% of trypsin activity. • Mesotrypsin, chymotrypsin c, and enzyme y can also lyse and inactivate trypsin. • These protease inhibitors are found in the acinar cell, the pancreatic secretions, In addition, low calcium concentration within the cytosol of acinar cells in the normal pancreas promotes the destruction of spontaneously activated trypsin. • Loss of any of these protective mechanisms leads to zymogen activation, autodigestion, and acute pancreatitis.
Exocrine-Endocrine Relationships • Insulin appears to be needed locally for secretin and CCK to promote exocrine secretion; thus, it acts in a permissive role for these two hormones. • Enteropancreatic Axis and Feedback Inhibition • The available evidence supports the concept that the duodenum contains a peptide called CCK-releasing factor that is involved in stimulating CCK release. • It appears that serine proteases inhibit pancreatic secretion by inactivating a CCK-releasing peptide in the lumen of the small intestine. • Acidification of the duodenum releases secretin, which stimulates vagal and other neural pathways to activate pancreatic duct cells, which secrete bicarbonate.
AcutePancreatitis • Pancreatic inflammatory disease may be classified as (1) acute pancreatitis or (2) chronic pancreatitis. • The pathologic spectrum of acute pancreatitis varies from interstitial pancreatitis, which is usually a mild and self-limited disorder, to necrotizing pancreatitis, in which the extent of pancreatic necrosis may correlate with the severity of the attack and its systemic manifestations.
Causes of Acute Pancreatitis • Gallstones (including microlithiasis) • Alcohol (acute and chronic alcoholism) Hypertriglyceridemia • Endoscopic retrograde cholangiopancreatography (ERCP), • blunt abdominal trauma • Postoperative • Drugs (azathioprine, 6-mercaptopurine, sulfonamides, estrogens, tetracycline, valproic acid, anti-HIV medications) • Sphincter of Oddi dysfunction
Hypertriglyceridemia is the cause of acute pancreatitis in 1.3–3.8% of cases. • Any factor (e.g., drugs or alcohol) that causes an abrupt increase in serum triglycerides to levels >11 mmol/L (1000 mg/dL) can precipitate a bout of acute pancreatitis. • Finally, patients with a deficiency of apolipoprotein CII have an increased incidence of pancreatitis; apolipoprotein CII activates lipoprotein lipase, which is important in clearing chylomicrons from the bloodstream. • Approximately 2–5% of cases of acute pancreatitis are drug related.
Several recent studies have suggested that pancreatitis is a disease that evolves in three phases. • The initial phase is characterized by intrapancreatic digestive enzyme activation and acinar cell injury. • Trypsin activation appears to be mediated by lysosomalhydrolases such as cathepsin B that become colocalized with digestive enzymes in intracellular organelles; it is currently believed that acinar cell injury is the consequence of trypsin activation. • The second phase of pancreatitis involves the activation, chemoattraction, and sequestration of leukocytes and macrophages in the pancreas, resulting in an enhanced intrapancreatic inflammatory reaction.
The third phase of pancreatitis is due to the effects of activated proteolytic enzymes and cytokines, released by the inflamed pancreas, on distant organs. • Activated proteolytic enzymes, especially trypsin, not only digest pancreatic and peripancreatic tissues but also activate other enzymes such as elastase and phospholipase A2. • The active enzymes and cytokines then digest cellular membranes and cause proteolysis, edema, interstitial hemorrhage, vascular damage, coagulation necrosis, fat necrosis, and parenchymal cell necrosis. • Cellular injury and death result in the liberation of bradykinin peptides, vasoactive substances, and histamine that can produce vasodilation, increased vascular permeability, and edema with profound effects on many organs, most notably the lung. • The systemic inflammatory response syndrome (SIRS) and acute respiratory distress syndrome (ARDS) as well as multiorgan failure may occur as a result of this cascade of local as well as distant effects.
There appear to be a number of genetic factors that can increase the susceptibility and/or modify the severity of pancreatic injury in acute pancreatitis. • Four susceptibility genes have been identified: (1) cationic trypsinogen mutations , (2) pancreatic secretorytrypsin inhibitor , (3) CFTR, and (4) monocytechemotactic protein (MCP-1). • Experimental and clinical data indicate that MCP-1 may be an important inflammatory mediator in the early pathologic process of acute pancreatitis, a determinant of the severity of the inflammatory response, and a promoter of organ failure.
Pancreatic SecretoryTrypsin Inhibitor (Psti) Gene Mutations • PSTI, or SPINK1, is a 56-amino-acid peptide that specifically inhibits trypsin by physically blocking its active site. SPINK1 acts as the first line of defense against prematurely activated trypsinogen in the acinar cell. • Recently, it has been shown that the frequency of SPINK1 mutations in patients with idiopathicchronic pancreatitis is markedly increased, suggesting that these mutations may be associated with pancreatitis.
Laboratory Data • The diagnosis of acute pancreatitis is usually established by the detection of an increased level of serum amylase and lipase. • Values threefold or more above normal virtually clinch the diagnosis if gut perforation, ischemia, and infarction are excluded. • Serum lipase activity increases in parallel with amylase activity. • A threefold elevated serum lipase value is usually diagnostic of acute pancreatitis; these tests are especially helpful in patients with nonpancreatic causes of hyperamylasemia.
Hypocalcemia occurs in 25% of patients. Leukocytosis occurs frequently. • Hyperglycemia • Hyperbilirubinemia [serum bilirubin >68 mol/L (>4.0 mg/dL)] occurs in 10% of patients. • Hypertriglyceridemia occurs in 5–10% of patients, • Finally, the electrocardiogram is occasionally abnormal in acute pancreatitis with ST-segment and T-wave abnormalities simulating myocardial ischemia.
Chronic Pancreatitis and Pancreatic Exocrine Insufficiency • Chronic pancreatitis is a disease process characterized by irreversible damage to the pancreas as distinct from the reversible changes noted in acute pancreatitis. • The condition is best defined by the presence of histologic abnormalities, including chronic inflammation, fibrosis, and progressive destruction of both exocrine and eventually endocrine tissue.
Causes • Alcoholic • Tobacco smoking • Hypercalcemia • Hyperlipidemia • Chronic renal failure • CFTR mutations • SPINK1 mutations • Isolated autoimmune chronic pancreatitis • Postnecrotic (severe acute pancreatitis) • Recurrent acute pancreatitis
alcoholism is the most common cause of clinically apparent chronic pancreatitis, while cystic fibrosis is the most frequent cause in children. • Recent investigations have indicated that up to 15% of patients with idiopathic pancreatitis may have pancreatitis due to genetic defects . mutations of CFTR. • This gene functions as a cyclic AMP–regulated chloride channel. • In patients with cystic fibrosis, the high concentration of macromolecules can block the pancreatic ducts.
Patients with chronic pancreatitis seek medical attention predominantly because of two symptoms: abdominal pain or maldigestion and weight loss. • In contrast to acute pancreatitis, the serum amylase and lipase levels are usually not strikingly elevated in chronic pancreatitis. • The diagnostic test with the best sensitivity and specificity is the hormone stimulation test utilizing secretin. It becomes abnormal when 60% of the pancreatic exocrine function has been lost. This usually correlates well with the onset of chronic abdominal pain.
Assessment of pancreatic function • Measurement of pancreatic enzymes : Amylase or alpha 1,4 –glucosidaseis the major enzyme which digests starch. The serum amylase contains the P ( pancreatic ) & S ( salivary) isoenzymes. These two can be distinguised by the inhibition test. Normal amylase level in serum is 50 – 120 Units.
The level rises within 5 hr of the onset of acute pancreatitis. • The level reaches a peak(4-6 fold) within 12 hours. • Within 2-4 days of the attack, the level returns to normal. • As the serum amylase level starts falling, urinary amylase level rises. • Amylase level in blood is mildly increased in cases of cholecystitis, peptic ulcer, diseases of mesentry & obstruction of intestine. • Chronic pancreatitis : no change or only mild elevation is noticed .
CLEARANCE RATIO : • If the sample is collected too early, the serum amylase levels may not show the expected rise. • If the sample is collected too late, again serum amylase may be low due to necrosis of the pancreatic tissue. • Calculation of clearance ratio will avoid these defects. CR = Urine amylase level x Scr x 100 Serum amylase level Ucr ( Scr & Ucr is serum & urinary creatinine level ) • In patients with acute pancreatitis, the ratio varies from 7-15%. • The normal ratio is 1-4.4%
serum lipase : • Major lipolytic enzyme which hydrolyzes glycerol esters of long chain fatty acids. • Normal level in serum : 30-235 U/L • The level in blood is highly elevated(2-50 fold) in acute pancreatitis.This persists for 7-14 days. • Thus lipase remains elevated longer than amylase. • Lipase is not elevated in salivary diseases. • Lipase estimation has advantage over amylase.
Macroamylasemia • In macroamylasemia, amylase circulates in the blood in a polymer form too large to be easily excreted by the kidney. Patients with this condition demonstrate an elevated serum amylase value, a low urinary amylase value, and a Cam/Ccr ratio of <1%. The presence of macroamylase can be documented by chromatography of the serum. The prevalence of macroamylasemia is 1.5% of the nonalcoholic general adult hospital population. Usually macroamylasemia is an incidental finding and is not related to disease of the pancreas or other organs. • Macrolipasemia has now been documented in a few patients with cirrhosis or non-Hodgkin's lymphoma. In these patients, the pancreas appeared normal on ultrasound and CT examination. Lipase was shown to be complexed with immunoglobulin A. Thus, the possibility of bothmacroamylasemia and macrolipasemia should be considered in patients with elevated blood levels of these enzymes.
The secretin test, used to detect diffuse pancreatic disease, is based on the physiologic principle that the pancreatic secretory response is directly related to the functional mass of pancreatic tissue. • In the standard assay, secretin is given IV in a dose of 0.2 g/kg of synthetic human secretin as a bolus. Normal values for the standard secretin test are (1) volume output >2 mL/kg per hour, (2) bicarbonate (HCO3–) concentration >80 mmol/L, and (3) HCO3– output >10 mmol/L in 1 hour. • The most reproducible measurement, giving the highest level of discrimination between normal subjects and patients with chronic pancreatic exocrine insufficiency, appears to be the maximal bicarbonate concentration.
There may be a dissociation between the results of the secretin test and other tests of absorptive function. For example, patients with chronic pancreatitis often have abnormally low outputs of HCO3– after secretin but have normal fecal fat excretion. Thus the secretin test measures the secretory capacity of ductular epithelium, while fecal fat excretion indirectly reflects intraluminallipolytic activity. • It must be noted that, an abnormal secretin test result suggests only that chronic pancreatic damage is present.
The amount of human elastase (normal level=175-1500µg/g of stool reflects the pancreatic output of this proteolyticenzyme. Decreased elastase activity in stool(<100 µg/g of stool) is an excellent test to detect severe pancreatic exocrine insufficiency in patients with chronic pancreatitis and cystic fibrosis provided that the stool specimen is solid. • The fecal elastase-1 and small bowel biopsy are useful in the evaluation of patients with suspected pancreatic steatorrhea. The fecal elastase level will be abnormal and small bowel histology will be normal in such patients.
Fat balance studies: • The astimation of fat in stool is done • When feces contains split fatty acids, it points to a normal pancreatic function,but defective absorption. • If fat excreated is neutral fat, is due to defective digestion, & is more in favour of pancreatic disease • Steatorrhea does not occur until intraluminal levels of lipase are markedly reduced, underscoring the fact that only small amounts of enzymes are necessary for intraluminal digestive activities. • Normal fat level in stool is • Children upto 6yrs of age -<2g/d • Thereafter – 2-6g/d • Steatorrhoea->7g/d
Estimation of sweat electrolytes • In pancreatic fibrocystic disease,sodium & chloride are increased in sweat. • The disease is characterized by thick viscous secretions of exocrine glands. • Sweat chloride levels of >60mmol/L,on two separate occations, is diagnostic of cystic fibrosis.