Prostrate Prostate
Prostrate Prostate. Brian Bizik MS PA-C. What are we going to cover ?. There is so much to cover, we have to be focused Daniel-son. I don’t know more than you, but over the last 3 months, I have spent more time reading, listening, talking etc about this topic than you. Hopefully.

Prostrate Prostate
E N D
Presentation Transcript
Prostrate Prostate Brian Bizik MS PA-C
What are we going to cover? There is so much to cover, we have to be focused Daniel-son. I don’t know more than you, but over the last 3 months, I have spent more time reading, listening, talking etc about this topic than you. Hopefully. So, let’s keep the big picture in mind as we examine this topic.
What are we looking for? • We want to know if they have any problem with the prostate at all, right? • Non-malignant • Malignant • Prostatitis – not going to cover but don’tforget about it
What are we looking for? • Two worlds here – very different. • On a good day . . . part of the urinary and genital systems
What is this thing anyway? • Normal gland about 20 grams – has capsule • Three zones, yes this is important.
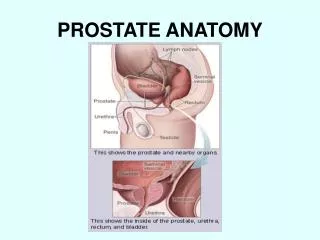
What is the function of the prostate? • The prostate is a male sex accessory gland that surrounds the urethra and contributes secretions to the ejaculate – SEE –we men accessorize! • It lies adjacent to the bladder and rectum, is surrounded incompletely by a thin capsule composed of collagen, elastin, and smooth muscle, and at the apex of the gland, forms part of the urethral sphincter apparatus • Nerves to the corpora cavernosa of the penis, needed for penile erection, travel through fascia along the posterolateral surface of the prostate and can often be preserved during radical prostatectomy to minimize sexual dysfunction postoperatively
This is our big picture! BPH Cancer Testosterone Tips AUA
Let’s define BPH • BPH is a nonmalignant enlargement of the prostate gland caused by cellular hyperplasia of both glandular and stromal (keep this term, stromal, in mind) elements that leads to troublesome lower urinary tract symptoms (LUTS) (in some men!) • It is the most common benign tumor in men and is not a precancerous condition
Common? Come on, you know it’s common 20% of men age 41-50 50% of men age 51-60 65% of men age 61-70 80% of men age 71-80 90% of men age 81-90 25-50% microscopic and macroscopic BPH will develop into clinical BPH The prevalence of clinical BPH in men ages 55-74 years 5-30% Only 40% of them have LUTS and only 20% seek medical advice
Ear hair, nose hair, prostate-they all just keep growing • Androgens • Estrogens • Lifestyle • Hereditary(genetic)/UnknownLet’s talk about this for just a second, these really matter for this talk!
Androgens • Testosterone and related hormones play a permissive role* in BPH • Androgens have to be present for BPH to occur • Administering exogenous testosterone is not associated with a significant increase in the risk of BPH symptomsSo, what happens to testosterone. . what is that strong kind of testosterone called???? *I don’t usually like “cute” medical sayings but Ilike this one - does not cause, but allows.
Androgens – Oh, yea, it’s called DHT • Didhydrotestosterone(DHT), a metabolite of testosterone is a critical mediator of prostatic growth. DHT is synthesized in the prostate from circulating testosterone by the action of the enzyme 5α-reductase, type 2. This enzyme is localized principally in the stromal cells; hence, these cells are the main site for the synthesis of DHT • In all prostate cell types, DHT binds to nuclear androgen receptors and signals the transcription of growth factors that are mitogenic to the epithelial and stromalcells. DHT is 10 times more potent than testosterone because it dissociates from the androgen receptor more slowly
Estrogen • Men with BPH often have higher levels of estrogen. Prostate tissue becomes more sensitive to estrogens and less responsive to DHT • Cells taken from the prostates of men who have BPH have been shown to grow in response to high estradiol levels with low androgens present • The true relationship is not clear and does not appear to be a linear one. . . dang estrogen.
Lifestyle • On a microscopic level, BPH can be seen in the vast majority of men over the age of 70 years, around the world but. . . . . • Men who lead a Western lifestyle have a much higher incidence of symptomatic BPH than men who lead a traditional or rural lifestyle. Do men in the West just whine more?
Pathological,first phase of BPH -asymptomatic and involves a progression from micro to macroscopic BPH Clinical or second phase of BPH - progression from pathological to ‘clinical BPH’ =development of LUTS Mechanical and dynamic components are responsible for the progression from pathological to clinical BPH In clinical BPH, the ratio of stroma to epithelium is 5: 1 Asymptomatic hyperplasia the ratio is 2.7:1 Path of BPH
Voiding/Obstructive symptoms: Hesitancy Intermittency Incomplete voiding Weak urinary stream Straining to pass urine Prolonged micturition Terminal dribbling (basketball) Bladder irritation symptoms: Frequency of urination Nocturia Urgency (compelling need to void that can not be deferred) Urge incontinence Lower Urinary Tract Symptoms-LUTS
Obstructive and irritative symptoms origin • Obstructive symptoms-mechanical obstruction due to glandular enlargement as well as dynamic obstruction secondary to contraction of the smooth muscle of the prostate, urethra and bladder neck. This dynamic obstruction is a result of sympathetic nervous system mediated stimulation of alpha-1adrenoceptors • Irritative symptoms - detrusor instability related to detrusor muscle changes in response to obstruction, such as bladder wall hypertrophy and collagen deposition in the bladder • OK, these adrenoceptors come in two types, can’t get into that here, no time. But I know that the 1A type are the majority in he prostate and 1D in the bladder. May need meds for one or the other depending on symptoms. So, one med may work better than another for any given guy. Don’t give up on these.
Treatment goals of BPH • Goal- rapid and sustained relief of symptoms: • Decrease bladder outlet obstruction • Improve bladder emptying • Lower detrusor instability • Reverse renal insufficiency • Prevent future episodes of gross hematuria, UTI and urinary retention • Quality of life and sexuality • Management depends on severity
Approach to a patient with BPH • History: LUTS, previous surgery in the GU tract, STD and Hx of urethral stricture. • Physical Examination :digital rectal exam to rule out nodules, asymmetry, hardened ridges, induration, bogginess, anal malignancy and detect problems with sphincter tone • Urinalysis- by dipstick and routine microscopy especially if symptomatic. Urine C&S to R/O infections and hematuria • Serum PSA-optional? to help detect cancer. More in a minute, I promise. • USE THE I-PISS!!
Mild (score 0-7) Moderate (score 8-19) Severe (score 20-35)IPSS.pdf – link to your own I-PiSS! IPSS – who said urologists had no funny bone
Treatment of BPH • Lifestyle modification • Watchful Waiting • Medical Therapy • Surgical Treatment : Conventional Surgical or Minimally Invasive Treatment
Lifestyle Changes • Enriched diet with ample amounts of fresh fish, fruits and vegetables, saturated fat reduction? • Reduce stress • Exercise on a regular basis • Weight within normal limits • Limit fluid intake, decrease bladder irritants-caffeine, alcohol; avoid anticholinergic drugs, narcotics and skeletal muscle relaxants • Seek txif you develop nocturia
Watchful Waiting • The risk of progression or complications is uncertain • In men with symptomatic BPH, progression is not inevitable some men resolve without tx • Some retrospective trials, inconclusive. Very few prospective studies addressing the natural history of BPH have been reported. The largest prospective study with finasteridevs. placebo in men with moderately to severely symptomatic BPH showed only 7% went on to acute urinary retention in 4 years. (McConnell et al, 1998).
Watchful Waiting • Appropriate management of men with mild symptom scores (0-7) • Men with moderate or severe symptoms can also be managed in this fashion if they so choose • Neither the optimal interval for follow-up nor specific endpoints for intervention have been defined
Medical Treatment • Alpha blockers • 5α-Reductase inhibitors • Combination Therapy
Initially used for treatment of high blood pressure The human prostate and bladder base contain alpha-1-adrenoreceptors and the prostate contracts to corresponding agonists. The contractile properties of the prostate and bladder neck are mediated primarily by the subtype α1a receptors Alpha blockade improves both objective and subjective symptoms and signs of BPH in some patients Alpha blockers can be classified according to their receptor selectivity as well as their half-life Alpha Blockers Oral Dosage Alpha-1 short-acting: Prazosin(Minipress)2mg BID Alpha-1, long-acting: Terazosin (Hytrin) 5 or 10 OD Doxazosin(Cardura)4 or 8 OD Alpha-1a selective: Tamsulosin(Flomax)0.4 or 0.8 OD Medical Treatment - Alpha blockers
Medical Treatment - Alpha blockers • Short Acting: Prazosin (Minipress) • Long-acting: Alfuzosin(Uroxatral), Doxazosin (Cardura) , Tamsulosin (Flomax) Terazosin (Hytrin) • Side Effects: dizziness, postural hypotension, fatigue, retrograde ejaculation, rhinitis, and headaches. May potentiate other antihypertensive medications • Studies have shown that all of them have comparable effectiveness • Terazosin and Doxazosinmay decrease the total cholesterol as well as LDL fraction. Both may cause first-dose syncope so titration is required • Alfuzosin and Tamsulosin-have alpha 1A selectivity and dose titration is not required • Don’t reduce the rate of cancer progression.
Medical Treatment - 5α-Reductase inhibitors • Finasteride (Proscar)is a 5α-reductase inhibitor that blocks that nasty conversion of testosterone to DHT. It affects the epithelial component of the prostate, resulting in a reduction in the size of the gland and improvement in symptoms • Six months of therapy are required to see the maximum effects on prostate size (20% reduction or more possible!) and symptomatic improvement • Symptomatic improvement mostly in men with quite large prostates • Side effects include decreased libido, decreased ejaculate volume, and impotence. • AND YES, Serum PSA is reduced by approximately 50% in patients being treated with Finasteride, but individual values may vary, thus complicating cancer detection
Medical Treatment - 5α-Reductase inhibitors • Dutasteride (Avodart): Some are concerned there is not enough data but class effect is likely according to AUA. In 3 double-blind trials it reduced acute urinary retention (1.8% versus 4.2%- placebo) and need for surgery (2.2% vs 4.1%) but increased impotence ( 7.3% vs 4.0%), ejaculation disorder, and gynecomastia and lowered libido • Cost is about double when I checked in September 2009at about $97 a month.
Medical Treatment - 5α-Reductase inhibitors • The reason you are here – the “eride” summary: • Yes, these meds reduce the progression to AUR and lowered the risk of a trip to the ER and a catheter. • Dutasteride may be a bit better on symptom control, not as much data though • Finasteride has a pretty good track record and both are generally well tolerated. • After 4 years. . . these meds AUR (NNT=26), Surgery (NNT=18), and prostate cancer! (NNT=17). But, if men are on these the risk of having the cancer found be a later stage cancer is a real one –number needed to harm. . . . . 77. What do we do?
Medical Treatment – Combo, SHORT TERM • Veterans Affairs Cooperative Study, 1229 men with BPH found Terazosinlowered the symptom score and increased the peak urinary flow rate when compared with placebo, Finasteridealone was no better than placebo and the combination of Finasterideand Terazosinwas no better than Terazosin alone • PREDICT trial in which 1095 men were randomly assigned to Doxazosin, finasterid or both for one year- Doxazosinmore effective than Finasterideor placebo for urinary symptoms and flow rate Combination no more effective than doxazosinealone • More trials show much the same • Conclusion: Combination treatment is beneficial for immediate relief of symptoms but may not be better at symptom relief than just the alfa blocker alone. Can start both thend/c the alpha once reductaseinhibitor has kicked in.
Medical Treatment – Combo, LONG TERM • Medical Therapy of Prostatic Symptoms (MTOPS) trial-3047 men with BPH randomly assign. to doxazosin, finasteride, combination therapy or placebo were evaluated for symptomatic improvement and overall clinical progression of the BPH. • Follow up at 4.5 yearscombination therapy reduced the risk of clinical progression (progression to an ER visit, surgery or other medical intervention) by 66 % • Symptom scores better with all therapies, but more with combined therapy • NNT to prevent one instance of overall clinical progression was 8.4 for combination therapy, 13.7 for doxazosin, and 15.0 for finasteride • Most side effects similar with mono or combo therapy except abnormal ejaculation, peripheral edema, and dyspnea, which were more common with combination therapy • Conclusion: Most studies found combo therapy better than mono therapy and made a stat sig difference after four years or more. Larger prostates and longer treatment times were predictive of a better drug impact.
Saw Palmetto Extract • American dwarf palm tree- the berries. The mechanism of action, if any, is unknown • Clinical trials- numerous but short and small sample size • 12-month randomized trial of saw palmetto in 225 men with moderate to severe BPH showed no evidence that saw palmetto is superior to placebo • A European study looked at Saw palmetto and finasteride in 1098 men with moderate BPH for 6 months found a decrease in IPSS to a similar degree 37-39%, improvement in QOL by 38-41% and increased urinary peak flow rates by 25-30 in both groups but the finasteride group had a significant worsening in sexual function scores compared with the Palmetto group. No placebo arm.
Saw Palmetto Extract • AAFP summary points out that half of European Urologists prefer this to regular meds. Oh, what do they know. • A Cochrane Review concluded that it does work, for those with mild to moderate symptoms. Comparable to Finasteride in fact. Oh, what do they know. • Hard to say at this point, AUA says not enough data, can’t recommend. . . . but can’t we add to watchful waiting?
Surgical Treatment • For patient who do not experience response to medical treatment in 12-24 months; for those whose symptoms progress, TURP(transurethral resection of the prostate) is the gold standard • A resectoscopeis introduced to the bladder and strips of prostatic adenoma are resected and dropped into the bladder. The prostate chips are extracted from the bladder and hemostasis is achieved with electrocautery • Under general anesthesia or with a regional block; 60-90 min. procedure. Requires 24-48 hours observation in hospital at most facilities.
Laser Therapy- A great option for some men now Green light laser- Just one type. Laser vaporization of prostate- causes rapid vaporization of the superficial tissue, with a minimal rim (2 mm) of coagulation Advantage: immediate TURP-like effect of the prostatic urethra, resulting in shorter duration of Foley catheterization in the initial post-op period Surgical Treatment
Robotic Surgery – quickly becoming a good option. Outcomes seem quite good. I don’t want to be unprofessional, but, butt, do you see anything wrong with the shape and layout of the surgery machine? Surgical Treatment
Do I have to? The DRE • Really no data to speak of. When the data that is available is combined, sensitivity is poor, at about 50%, and typically with larger cancers. • One major trial looking at all the numbers says that 72-82% of men who have a biopsy based on DRE alone will not have cancer. That is a lot of procedures for a cancer that may not even hurt you. Controversial, uh, so I won’tput my finger there any more!!
Do I do a PSA or not, just make up your mind. • PSA is a glycoprotein from normal and neoplastic tissue. • Originally used to track cancer, it’s widespread use in the late 1980’s led to a dramatic rise in prostate cancer diagnosis. • Lots of fancy bias types in PSA studies. • The Prostate Cancer Prevention Trial found that men, without symptoms, and with low PSAlevels still had cancer 15.2% of the time.
Do I do a PSA or not, just make up your mind. • PSA levels DO show a fairly good linear relationship with cancer rates. The end numbers are that overall the test has a 72% sensitivity and 93% specificity (meta analysis from AAFP) • The numbers above agree with Cochrane summaries with say this: 38% or about a third of all prostate cancers occur in men withPSA levels considered normal (less than 4!)
Evidence is insufficient to recommend for or against Offer DRE and PSA to >50 y, LE of 10+ y, black men at 45 y. YES! Offer DRE and PSA to all men over 50 and 10+ LE PSA testing, what do the experts say? AAFP ACS AUA Evidence is insufficient torecommend for or against but not after age 75 USPSTF
Best single slide of the conference!! There are things you can do to make the PSA test better! Do this and be at the cutting edge of prostate health care!! Lower PSA cutoff values for younger men. Over 2.5 ng per ml is too high for men 40-50 years. Ratio o free-to-total PSA goes down in cancer. If % free is 0-10, rate is 58%, 10-15, 28%, 15-20, 20%, 20-25, 16%. PSA Velocity! Greater than a 0.5 ng per ml rise in one year is too fast, f/u of some kind needed.
Quick Review so far. . . . • BPH (Benign prostatic hyperplasia) becomes increasingly common as men age • Many men with BPH are asymptomatic or have only mild symptoms, and may not require therapy • Alpha-adrenergic antagonists provide immediate therapeutic benefits and are first line treatment for smaller prostates and mild symptoms • 5-alpha-reductase inhibitors require long-term treatment for efficacy and are beneficial for larger prostates and mild to moderate symptoms • Combined therapy often better • DRE and PSA’s have limits, but doing them with some additional tips may make them worth it
This is our big picture! BPH Cancer Testosterone Tips AUA
Hypogonadism – what did you call me? • A decrease in either of the two major functions of the testes: • sperm production • testosterone production
Hypothalamic-Pituitary-Testis Axis Inhibin B