Download
1 / 43
430 likes | 564 Vues
Primary Prevention of Birth Defects by Periconceptional Folic-Acid Containing Multivitamin Supplementation. Prof. Andrew E. Czeizel, MD., C.Sc., D.Sc. (Scientific director of the Foundation for Community Control of Hereditary Diseases, Bu dapest, Hungary) Dr. Attila Vereczkey, M.D., M.A.

E N D
Primary Prevention of Birth Defects by Periconceptional Folic-Acid Containing Multivitamin Supplementation Prof. Andrew E. Czeizel, MD., C.Sc., D.Sc.(Scientific director of the Foundation for Community Control ofHereditary Diseases,Budapest, Hungary) Dr. Attila Vereczkey, M.D., M.A. (Medical Director of the Versys Clinics, Human Reproduction Institute, Budapest, Hungary)
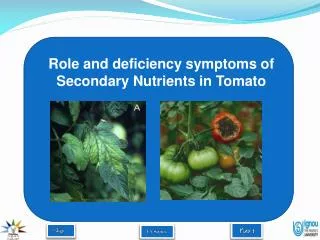
The deficiency or overdosage of certain nutrients may have a role in the origin of birth defects. • First in 1932 Fred Hale demonstrated that a vitamin A-free diet during early pregnancy of sows resulted in offspring without eyeballs, oral clefts, accessory ears, malposition of kidney and defects of hind legs.
Joseph Warkany (1902-1992), known as „ father of teratology”, recognized the importance of purified diets and used these to test various vitamin deficiencies for their teratogenic effects. • Warkany found that maternal dietary deficiency can induce structural birth defects, i.e., congenital abnormalities (CAs).
Richard W Smithells (1924 - 2002) MD, FRCPCH, FRCP, FRCPE, FRCOG, DCHProfessor of Paediatrics and Child Health, 1968-1988 • In 1964 Hibbard reported a higher rate of CAs (3%) in the infants of folate-deficient mothers than in controls (1.6%) • Hibbard and Smithells showed a relationship between human embryopathy and a deficiency of folate metabolism • Smithells et al demonstrated the role of vitamin deficiencies in the origin of neural-tube defects (NTD). • He was the first who hypothesized that among triggering environmental factors in the origin of NTDs, undernutrition could be the common and major denominator.
NTD: spina bifida aperta NTD: spina bifida cystica 3/a 3/b
Characteristics of NTD • Origin of isolated NTDs (92% of all cases) can be explained by gene-environmental interaction. • Polygenic predisposition: fact that recurrence in first degree relatives is 10 times higher than their occurrence • Environmental factors: very wide range (0.5-12 per 1000) of NTD incidences in different populations, rapid secular changes and seasonal variation of births with NTD’s were observed. Socio-economic status dependence (a low risk in the highest class to an above-average risk in the lowest class) which was found in several populations • Early critical period: between 15th and 28th postconceptional days, this explains the use of "periconceptional supplementation". • Estimated annual number of cases affected with NTD throughout the world is about 400,000
Periconceptional vitamin supplementation: • Commence 28 days prior to conception • Continue until the second missed MP 21-26 days conception Closure of neural tubes menstruation
Hungarian Periconceptional Service (HPS)1984. • The Hungarian Periconceptional Service (HPS) was launched in 1984 by A.E.Czeizel. • It embraces all the ethods for the prevention of structural birth defects(i.e. congenital abnormalities) and pre-term birthknown at that time. • prefer to use the term “periconceptional” rather than “preconceptional” • The most sensitive and vulnerable early period of fetal development, is not covered by the standard medical health service, leaving embryos uncared for and in general unprotected Prof. A.E. Czeizel
The three stages of the Hungarian Periconceptional Service, and activities undertaken at each stage • 1) Reproductive Health check-up • a) Family history of prospective mother and father, and obstetric history of females. • b) Case history and available medical records of females, e.g., epilepsy, diabetes, • c) Vaginal and cervical smear screening for sexually transmitted infections/disorders. • d) Sperm analysis to detect subfertility and pyosperm (i.e. pus cells in the semen as indicators of sexually transmitted infections) • e) Psychosexual assessment. • f) Blood screening of women to detect rubella seronegativity, or lack of previous exposure to varicella (vaccination will be offered), or HIV positivity. In addition, carrier screening for cystic fibrosis, and, more recently, predictive genetic diagnostic tests are carried out at this stage.
The three stages of the Hungarian Periconceptional Service, and activities undertaken at each stage • 2) The 3-month preparation for conception period • a.) Protection of germ cells: avoidance of tobacco, alcohol or narcotic consumption, and taking of unnecessary drugs. • b) Discontinuation of oral contraception, and removal of IUDs (condoms are provided). • c) Occupational history of females • d) Menstrual history; measurement of basal body temperature for detection of hormonal dysfunction (and commencement of further investigation and treatment, if necessary). • e) Start of pre-conceptional multivitamin supplementation. • f) Recommendation that dental status be checked. • h) Guidelines for physical exercise. • i) Guidelines for healthy diet
The three stages of the Hungarian Periconceptional Service, and activities undertaken at each stage • 3) Better protection of early pregnancy • a) Undertaking of all additional investigation/treatment necessitated by conditions and disorders detected at the pre-conception check-up. • b) Appropriate investigation and treatment of women shown to suffer from hormonal dysfunction • c) Optimal timing of conception in relation to ovulation. • d) Early pregnancy confirmation using pregnancy tests and ultrasound scanning. • e) Post-conceptional multivitamin supplementation. • f) Avoidance of teratogenic and other risks. • g) Referral of pregnant women to prenatal care clinics.
Data and Results of Previous Intervention Studies for the Reduction of Recurrent NTD Based upon the results of the MRC Vitamin Study, the Centers for Disease Control (CDC) in 1991 recommended daily supplementation of diet with 0,4 mg of folic acid under medical supervision in the periconception period for women at high risk (i.e. who had one or more previous offspring with NTD) for the reduction of NTD recurrence. 19. Smithells RW, Sheppard S, Schorah CJ, et al. Possible prevention of neural tube defects by periconceptional vitamin supplementation. Lancet 1980; 1: 339-340. 20. Smithells RW, Sheppard S, Wild J, Schorah CJ. Prevention of neural tube defect recurrences in Yorkshire: final report. Lancet 1989; 2: 498-499. 21. Nevin NC, Seller MJ. Prevention of neural tube defect recurrences. Lancet 1990; 1: 178-179.
Goals of the Hungarian randomized double-blind controlled trial (RCT) About 95% of women with NTD offspring have no previous NTD pregnancies. - Thus the question is whether the periconceptional folic acid- containing multivitamin supplementation can reduce the firstoccurrence of NTD? The pharmacological dose (> 1 mg, e.g., 4 mg) of folic acid cannot be recommended for the population at large or without medical supervision. - Thus, the question is whether a physiological dose (< 1 mg) is effective or not? Possible other beneficial or adverse effects of periconceptional multivitamin supplementation.
Result of the Hungarian RCT: Reduction of the First Occurrence of NTD
Based upon the Hungarian RCT and some observational studies, the CDC in September 1992 recommended that "all women of childbearing age who are capable of becoming pregnant should consume 0.4 mg of folic acid per day for the purpose of reducing their risk of having a pregnancy affected with spina bifida or other NTD” and this recommendation was subsequently followed by several countries. • CDC. Recommendations for the use of folic acid to reduce the number of cases of spinabifida and other neural tube defects. MMWR 1992; 41: 1233-1238.
Number and rate (per 1000) of different CA-groups in multivitamin and no multivitamin supplemented group
OTHER EXPERIENCES OF THE HUNGARIAN RANDOMIZED CONTROLLED TRIAL • Female cycle become more regular • No difference between sexual activity • 7% higher rate of conceptions • Time to become pregnant was slightly but significantly shorter • Significantly lower rate of severe morning sickness, neusea vomiting in pregnancy (3,0 vs 6,6%) • No difference in maternal weight gain • Constipation (1,8 vs 0,8%) diarrhoea (1,4 vs 0,4%) more often • Multiple birth was 40% higher in multivitamin group • No significant difference in fetal deaths ( biochemical PR, ectopic PR, miscarriages, stillbirths), somewhat higher in multivitamin group ( no terathanasia- multiple PR) • Sex ratio showed slightly girl excess vs 51% boy predominance • No difference in gestational age at birth, and birth weight • No difference in postnatal somatic and mental development until 6 yrs
Supplemented cohort: Participants of the Hungarian Periconceptional Service (HPS) with the same multivitamin use(0.8mg folic acid), until 14th week of gestation No. of participants: 3056 Unsupplemented cohort: Participants of regional Antenatal care, matched to age socioeconomic status and region, without folic acid /multivitamin supplementation use after 14th week of gestation 3056 Hungarian Cohort-Controlled Trial ( CCT ) of Periconceptional Multivitamin Supplementation
Reduction of NTD by periconceptional folic acid-containing multivitamin supplementation in two Hungarian intervention studies 0.06 (0.04,0.13) 0.11 (0.01,0.91) 0.08 (0.01,0.47)
Number of informative offspring with cardiovascular CAs in multivitamin (MV) and no multivitamin (No-MV) groups
Number of informative offspring with urinary tract’s CAs in multivitamin (MV) and no multivitamin (No-MV) groups
Number of informative offspring with other „candidate” CAs in multivitamin (MV) and no multivitamin (No-MV) groups
Other observational studiesregarding periconceptional (folic acid containing) multivitamin supplementation “Other” CAs Association confirmed refused Cardiovascular CAs 5 1 CAs of urinary tract 3 0 Congenital limb deficiencies 3 0 Congenital pyloric stenosis 0 1
Vitamin B Proteins 11 Folate Folic acid (polyglutamate) (monoglutamate) Conjugase Zinc Monoglutamate Reductase Methionine Dihydrofolate Reductase S-adenosylmethionine CH 3 Tetrahydrofolate = + Serin CH THF Methionine- 3 Vitamin C synthase Cystathione-beta 5,10-methylene-THF B Homocysteine 12 synthase 5-methyl-THF Homocysteine B 6 Cystathione Methylene-THF- reductase=MTHFR Cystathionase Homocystinuria B B 6 Cysteine 2 MTHFR-gene Sulphate Metabolism of Homocysteine and the Effect of Folate-Folic Acid (Vitamin B11), Vitamin B2, Vitamin B6and Vitamin B12
MTHFR gene Gene location: Chromosome 1, short arm 36.3 Mutation: 677 C T Frequency of mutant homozygosity (TT): 5-15 % (11%) heterozygosity (CT): 25-65% (45%)
Optimal Dosage ? Good 400 microgram of folic acid Better 800 microgram of folic acid Best Multivitamin containing 800 microgram folic acid
Comparison of different preventive approaches of NTD * incl. termination of pregnancy
Conclusion I:Periconceptional multivitamin (containing 0.8 mg folic acid) supplementation 1. Very effective (about 90%) for the prevention of NTD 2. Effective for the reduction of cardiovascular CAs (ventricular septal defect), CAs of urinary tract (stenosis/atresia of pelvicureteric junction) and congenital limb deficiencies (terminal transverse type) 3. No effective for the prevention of orofacial cleft (dose-dependent effect of folic acid alone?) 4. Effective for the reduction of total (birth+fetal) prevalence of major CAs at least by one-third
Conclusion II: • Neural-tube defects are preventable by periconceptional folic acid or multivitamin supplementation. • The incidence of some other structural birth defects can also be reduced by folic acid-containing multivitamin use during the periconception period. • All women of childbearing age who are capable of becoming pregnant should consume folic and/or folic acid containing multivitamin during the periconception period. • The primary prevention of birth defects by periconceptional folic acid/multivitamin supplementation is much better than the so-called secondary prevention, i.e. the termination of pregnancy due to severe fetal defects. • Periconceptional care – beyond other benefits – is optimal for the introduction of periconceptional folic acid/multivitamin supplementation. • Proper preparation for conception is the earliest and most effective method for the prevention of birth defects.
Thus G. P. Oakley is right: “Inertia on folic acid fortification equals public health malpractice”. Oakley GP. Inertia on folic acid fortification: Public health malpractice. Teratology 2002; 66: 44-54.
Environmental Sciences Lifestyle Sciences Nutrition Dietetics Toxicology Teratology Pharmacology Biotechnology Genetics-Epigenetics Assisted Reproductive Technologies Embryology Psychology The founding of the first World Scientific Society of Periconeptional Medicineis under process! International Society of Periconceptional Medicine ISPM Register online: www.ispm.org
Thank you for your attention! 1st world congress of the ISPM in Budapest, Hungary, 2012 !! ispm2012
Preventive efficacy of folic acid alone 70% ? Key factor Low multivitamin 90% At least three other CA-groups Vitamin B12, B2 and B6 are independent factors Moderate (reimbursement) NTD Other CAs Other arguments in hyperhomocysteinemia related NTD Cost
Cardiovacular defects: Government of Western Australia, WA Register of Developmental Anomaliessource: Department of Health, AU
Chromosomal defects: Government of Western Australia, WA Register of Developmental Anomaliessource: Department of Health, AU
NTD trends: Government of Western Australia, WA Register of Developmental Anomaliessource: Department of Health, AU
NTD trends: Government of Western Australia, WA Register of Developmental Anomaliessource: Department of Health, AU