Download
1 / 20
240 likes | 382 Vues
Learn about the impact of PEG feeding on adult patients' daily life and QoL from patients' and carers' perspectives.

E N D
The Impact of Percutaneous Endoscopic Gastrostomy Feeding upon Quality of Life in Adults Ailsa Brotherton Senior Research Fellow (ambrotherton@uclan.ac.uk)
Small group discussions • What is QoL? • Define QoL in one sentence • Discuss the factors that are important to your QoL.
QoL QoL is a dynamic construct which is constantly being negotiated by the individual in association with his/her environment and those around him. Health Related Quality of Life (HRQoL) Meaningful measure of the health related issues associated with an individual’s QoL e.g. measures of the impact of symptoms and treatment interventions.
Introduction of the paper This paper is part of a larger research project which: • Included a pilot study to measure QoL of adult patients on a PEG using the SF36 • Developed a semi structured interview approach to explore the issues and concerns of living with a PEG and the impact upon daily life in 3 subgroups (adult patients, carers of adults, carers of children) • Compared the perceptions of health care professionals with those of patients and their carers • Developed a preliminary PEG QoL assessment tool
Background • Very few studies have been reported that formally measure QoL in the PEG population Loeser et al, 2003 assessed QoL by proxy rating and self-rating: Karnofsky and Spitzer indices (purely functional scales) European Organization for Research and Treatment of Cancer [EORTC] QLQ C30 Concluded: QoL is reduced in patients on HETF, partly explained by malnutrition. (Schneider et al, 2000;Roberge et al, 2000; Klose et al, 2003) • The available QoL measures are not specifically designed to measure the impact of feeding on QoL and do not contain questions to determine this • No known validated QoL assessment tools that have been developed and validated specifically for patients with a PEG • Numerous methodological difficulties in measuring disease specific health related QoL (Abbott, Webb and Dodd, 1997, Abbott and Gee, 2003)
Aim • To understand how the provision of enteral feeding via a PEG impacts on the daily life and QoL of adult patients, from both the patients’ and carers’ perspectives • Approval was obtained from the Local Research and Ethics Committee and informed consent was sought.
Methods • Cross sectional qualitative design • Purposive sampling • Semi-structured interview approach developed to provide a consistent framework of questions for the patients and carers Semi-structured interviews • Format developed based on: Available literature regarding patients’/carers’ views of PEG feeding Personal experiences of clinical practice Discussions with HCP’s in the field. • Open and closed questions falling broadly into two categories: Service provision Impact of feeding on daily life • Eligibility: All adult patients receiving enteral feeds via a PEG within an NHS Trust, in the Northwest of England.
Data collection and analysis Data Collection • Subjects: 15 adult patients 19 carers of adults • Location: subject’s choice - primarily own homes, some hospital. • Interviews: All taped except in 2 patients who could not speak – communication aids were used and their own words were documented exactly as written Data analysis • Interviews transcribed and analysed manually: • Open questions: Systematic searching for relevant phrases Extracting and coding of phrases Sequential stages of reduction and ordering Identification of emerged themes • Closed Questions: Results presented as percentages of the responses given. • Independent analysis of one third of the transcripts by second researcher
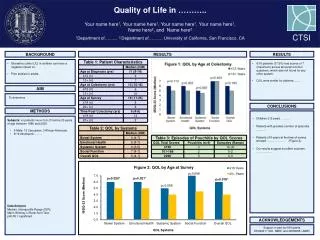
Results: responses to closed questions Do you experience any difficulties administering the feed? Are you happy with the feeding regimen?
In your view, do you (the patient) have an acceptable QoL? Results cont. Do you receive sufficient support from the HCP’s?
Ranking of the questions by propensity to generate disagreement and estimated odds for relationships Questions 3 and 4 generate similar perceptions between respondents. Differences in perceptions are greater for Questions 5, 2 and 8 The differences in perceptions are greatest for Questions 7, 6 and 1. * The odds are the relative odds of disagreement to non-disagreement. Hence odds of 0.18, for example, imply 18 disagreements for every 118 adults with PEG and hence a probability of 18/118 = 0.15. Similarly odds of 0.02 imply 2 disagreements for every 102 adults, giving 2/102 = 0.02.
Implications for clinical practice • The effect of role pairing was significant (p<0.025). • Broadly speaking: • Disagreement between a carer and a health care professional is estimated at one and a half times as likely as between two health care professionals. • The gap in perceptions between patient and professional is larger with patient and professional estimated as two and a half times as likely to disagree as two professionals. • Perhaps even more surprising, the largest gap in perceptions is between the patient and their carer, since the patient and their carer are estimated almost three times more likely to disagree compared with two professionals.
Emerging themes from open questions: the impact of feeding on daily life • Relief of pressure to eat at mealtimes ‘It has taken the pressure off mealtimes; I was finding it very difficult to eat. I was spending hours on each meal and not finishing it’ • Disturbed sleep It disturbs my sleep so much. When you go to bed and this tube is just sticking out of your stomach: you cannot move’ • Restricted ability to go out ‘Well, I just don’t go out anymore’ ‘Well I have to be here all day everyday; one carer comes in to sit with him for 2 hours a week while I go and do my shopping’ ‘Everything about his regimen restricts my life. He’s feeding during the day now and it is stopping us from going out. I’m quite bitter about it because he hasn’t got that long to live’ • Restricted choice of clothes/leakage of feed on clothes ‘I can’t wear a bikini or cropped tops on my holidays like all my friends’ ‘It permanently leaks; I have to cover up and wrap up though you can’t afford to let it affect you, life’s too short to be self conscious’ • Difficulties finding a place to feed ‘I gave him the feed on a bench in town once and I vowed I would never do that again’
Themes cont… • Missing food / drinks ‘I just miss eating and drinking’ ‘I only cook dishes that I know he didn’t like .I couldn’t sit and eat his favourite meal while he cannot have even one mouthful’ • Social occasions: Christmas, birthday parties ‘It affects your social life when you go to parties. I go but I feel alienated and other people feel uncomfortable because they are eating and I cannot’ ‘We can’t even have a drink together at Christmas or even a piece of cake or a cup of tea. I don’t like drinking in front of him because I know he would love a cup of tea’ • Negative attitudes of others towards feeding ‘If we are in a restaurant people can be really put off’ ‘My husband is frightened of the tube; he’s frightened to give me a hug’ • Burden placed on other family members ‘Fancy getting to seventy six and having to get up at six every morning (to let the carers in). I would welcome that Shipman here. I would if he had two lethal injections, one for him and one for me’
Depression Anger Frustration Relief Fear Worry Gratitude Carers only Upsetting Queasiness Feelings towards PEG feeding
Conclusion • Wide range of patient and carer experiences and perspectives • Cannot generalise about the impact of PEG feeding on individual patients and their families • Increased social support / support for daily life required, planned on an individualised basis • Need to develop objective way to measure the impact of PEG feeding on QoL Further planned research • Psychometric validation of the PEG QoL tool for the 3 subgroups: Adult patients, carers of adults, carers of children
Acknowledgements • Sincere thanks to: • The patients and carers who participated. • My supervisory team: Professor Janice Abbott - Director of Studies Professor Peter Aggett - Second supervisor • Seedcorn Funding Committee/ NHS Trust
References • Loeser,C, von Herz U, KÜchler T, et al. Quality of Life and Nutritional State in Patients on Home Enteral Tube Feeding. Nutrition.2003. Vol 19,605-611. • Klose J, Heldwein W, Rafferzeder M, et al. Nutritional Status and Quality of Life in patients with Percutaneous Endoscopic Gastrostomy (PEG) in practice. Prospective one-year follow up. Digestive Diseases and Sciences. 2003. 48, No 10; 2057-2063 • Schneider SM, Pouget I, Staccini P, et al. Quality of Life in long-term home enteral nutrition patients. Clinical Nutrition. 2000. 19 (1): 23-28 • Roberge C, Tran M, Massoud C, et al. Quality of life and home enteral tube feeding: a French prospective study in patients with head and neck or oesophageal cancer. British Journal of Cancer. 2000. 82 (2) 263-269 • Abbott J, Webb AK, Dodd M. Quality of Life in Cystic Fibrosis. Journal of the Royal Society of Medicine, 1997; 90: 37-42. • Abbott J, Gee L. Quality of Life in Children and Adolescents with Cystic Fibrosis: Implications for Optimising Treatments and Clinical Trial Designs. Paediatric Drugs, 2003; 5(1): 41-56.