Addressing the Human Resource Crisis in Ghana’s Health Sector: Strategies and Challenges
Ghana's healthcare faces a critical human resource crisis due to out-migration and skewed distribution of health workers. With over 22 million people and 55% living in rural areas, the country struggles to provide equitable healthcare access. Current policies aim to address this through training, incentives, and restructuring, but challenges remain. Understanding the root causes, including globalization effects and poor working conditions, is essential for developing effective solutions. Continuous engagement with health workers and communities is critical in shaping impactful health policies.


Addressing the Human Resource Crisis in Ghana’s Health Sector: Strategies and Challenges
E N D
Presentation Transcript
Introduction and structure • Ghana faced HRH crisis (out migration and distribution) • Policy measures to address the crisis... • Approach without evidence and involvement of HW and communities • Ghana /structure of health services • Out-migration/ what has been done? • Evidence of mal-distribution (effects) • What has been done to address it? (Results?) • What needs to be done to address it?
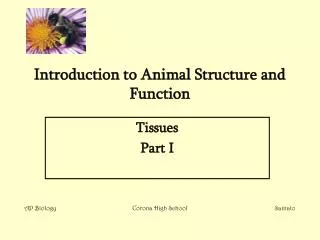
The Regional Map of Ghana • Area of 238,537 sq.km. • Population of over 22 million • 55% of the people live in rural areas • Agriculture accounts for 41% of GDP and employs 60% of the workforce • GDP per capita US$ 2,130 in (2002) • 10 administrative regions • Decentralised local government structures • Located on the west cost of Africa
Organisation of Ghana’s Health Care System • Health policy serves as the engine for wealth creation • Three tier levels operating on preventive and curative models of health care • - Primary care (CHPS, Health centres, clinics, maternity homes) • - Secondary care ( districts, metro, municipal, regions) • - Tertiary (teaching hospitals, research Inst.) • MOH- policy, resource mobilisation, coordination • Training & Research- HTI, Universities, Research Institutions • Service Delivery- GHS, TH’s Mission, Quasi, Private, Ghana Ambulance Service, TAMP • Regulation - MDC, PC,NMC,FDB, PHMBH,TAMPC • Financing - NHIA, GOG, Partners
The size of public health workforce39,000 in 2003 to 46,000 in 2009
What we know about out migration and rural practice • Continuing Demands on Health Workers from Developed Countries -effects of Globalization -large unmet HRH needs of developed countries. -attractive pay regimes • The Push Factors -years of under-investment in human resource, (production & dev’t) - poor conditions of service - restrictive employment policies - poor working environment (lack of equipment, etc) • Effect of HIV/AIDS on HRH - rising employee attrition, - increasing absenteeism, - low productivity • Effect of out migration on rural practice – Highly skilled health workers move to urban areas to fill vacancies as a result of relatively attractive conditions in urban areas. (social, environmental, facility, equipment, education)
HRH Policy to address ‘out migration’ • HRH Education, Training and Development : - focus on the training of middle level health workers - increase intake into Training Institutions & skill mix - encourage the private sector participation in training HRH • Establishment of Ghana College of Surgeons and Physicians: - localized postgraduate training - Enhanced professional and career development, through fellowships • Strengthening systems and structures -accreditation and regulation - Infrastructure development • Salary rationalisation (2006) • Incentives (car loans, housing schemes, tax exemptions) • MIDA/GHANA health project ( ‘brain gain’ through short term exchanges) • Ghana Health Workforce Observatory
HRH policy on training focuses on the production of middle level health workers. HRH policies have been structured to increase training and recruitment of more clinical health workers as against support staff
Today, HRH challenges remain - progress in modern medicine - production of new drugs and new ways of medical investigations - new devices and new ways of using them - new skills and competencies in the use of complex tools and equipment - personnel trained in narrow fields - patients seeing variety of health care providers - Increasing demand on health care
The problem with HRH in rural Ghana...... • In Ghana, the effect of global HRH challenges affected equitable distribution of qualified health workers. • lack of appropriate skills to perform the needed tasks • The distribution of qualified health workers are skewed highly in favour of the urban areas. • Those areas therefore depend mostly on auxiliary staff for service delivery.
Measures adopted in the past to retain health workers in rural areas.... • Deprived area incentives (25% of basic salaries) • Compulsory posting • Fast track promotions • Decentralisation of HRH • Fellowships However, these measures failed/not properly implemented to address the challenges
Now let us pause, reflect and look for the evidence! • “We were not sent into this World to do anything into which we cannot put our hearts” …….John Ruskin (1819-1900) A famous English author, Poet and Social Critic
WHO recommends 2.43 of clinical health workers like Nurses, Midwives and Doctors for countries to attain 80% coverage of deliveries Density of Doctors, Nurses and Midwives:
Outpatient attendance and HRH implications In 2001, the out-patient attendance per doctor: - in a typical teaching hospital was 1805 - in a regional hospital was 5341. During the same period, the out-patient attendance per nurse: in a teaching hospital was 404 in a regional hospital was 963
Varied Staffing ratios • Average doctor; bed ratio =0.05 • Average nurse; bed ratio = 0.64 • Varied staffing ratios; Doctors ranges from 0.20 in urban areas to 0.01 in rural areas; Nurses ranges from 1.36 in urban areas to 0.21 in rural areas
Health workers and rural practice • Rural practice of qualified health workers has historic and global dimensions • Chris Ham (1982) from Butler et al (1973) indicated that in Britain, ‘areas which are currently facing most serious shortages seem to have a fairly long history of manpower difficulties.......’ ( Butler, Bevan and Taylor,1973, p 42)
Engaging the workers/communities Addressing R&R in Rural areas Establishing The problem From evidence Show impact of Problem on Health outcomes By engaging Workers, communities Identify factors Affecting R&R Rural areas; What are the Factors that Can improve situation Change old factors not working (adopt realistic Ones) • Org. Structure • Policy • Social environment • H/Reforms • HR systems • HR management • Motivation • Economic models • Labour market • Demand/supply Contribute to improvements in health outcomes
What the literature says? • Internationally, there is evidence that higher density of HRH is a significant factor in improving maternal, infant and under-five mortality rates (Anand et al, 2004) • There is ecological evidence of positive correlation between pop density of HRH and cost effective health interventions (Speybroeck et al 2006) • HRH play a critical role in improving health outcomes - adequate health care depends on the availability of health workforce (WHO, World Bank reports, 2006) • In all countries shortage of qualified health professionals is more critical in rural or underserved areas (Dussault, G and Franceschini, M, 2006) • Geographical mal distribution of qualified health workers exacerbates the existing inequalities and contributes to lower health outcomes in rural areas (Hayes et al 2005)
Methods/Techniques/analysis • Action research to diagnose the problem • A randomized sample size of 42health workers making 5.5% of workers in those districts (MD’s, Nurses, Pharmacists, Allied Health professionals) and 8 (students, heads of Training Institutions, policy makers and community leaders) from 6 rural districts • Smaller groups of 8 formed for focus group workshops to solicit views about the scope of the problem and consequent health impact • Smaller groups analysed the views and prioritised them
Health workforce shortage in rural areas is critical than previously estimated • While most of the urban areas are operating at a maximum HRH capacity, there are gaps in HRH ratios in rural areas • There are no significant differences in medical doctor density and three health outcomes between government classified deprived regions and the other regions • Health care delivery is a team work and requires effective skill mix
Findings • Increased workload, stress, low productivity • Existing policies on recruitment and retention were formulated without the involvement of workers and communities • Involving stakeholders in problem diagnosis ensures greater sense of awareness • Impact of problem is greatly felt if methods employed involve the people • Communities are willing to support interventions if involved in problem diagnosis
Policy implications • Since previous attempts to equitably distribute have proved unsuccessful, there is the need to explore obstacles and barriers to improvement • Realising the impact on health outcomes, there is the need to identify what constitute realistic incentive package in underserved areas • What policy steps are needed to support change • Critical need to explore means of attracting and retaining qualified health workers to rural or underserved areas in Ghana in order to effect significant change in health outcomes.
“Together, we train and deploy forces to combat the disease burden and disabilities in our society today”………….. That is our health workers , motivated and retained at all levels! • Thank you