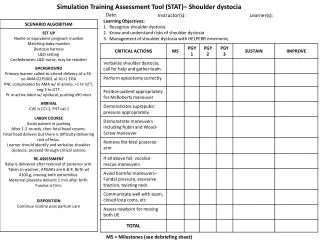
RNR Simulation Tool
RNR Simulation Tool. Phillip Barbour Master Trainer for Center for Health and Justice at TASC (CHJ). Risk, Needs, Responsivity (RNR) and Recidivism: An Update on Theory. Center for Advancing Correctional Excellence (ACE!) George Mason University www.gmuace.org/tools.

RNR Simulation Tool
E N D
Presentation Transcript
RNR Simulation Tool Phillip Barbour Master Trainer for Center for Health and Justice at TASC (CHJ)
Risk, Needs, Responsivity (RNR) and Recidivism: An Update on Theory Center for Advancing Correctional Excellence (ACE!) George Mason University www.gmuace.org/tools • BJA: 2009-DG-BX-K026; BJA: 2010-DG-BX-K077; SAMHSA: 202171; Public Welfare Foundation
Faye S. Taxman, Ph.D University Professor Center for Advancing Correctional Excellence Criminology, Law and Society George Mason University 10519 Braddock Road Suite 1900 Fairfax, VA 22032 James M. Byrne, Ph.D. Professor University of Massachusetts, Lowell Griffith University April Pattavina, Ph.D. Discrete Event Model Associate Professor University of Massachusetts, Lowell AvinashSingh Bhati, Ph.D. Simulation Model Maxarth, LLC Michael S. Caudy, Ph.D. Stephanie A. Maass, M.A. Erin L. Crites, M.A. Lauren Duhaime, B.A. Amy Murphy, MPP Joseph Durso, M.A. Gina Rosch Special Acknowledgements: • Bureau of Justice Assistance • BJA: 2009-DG-BX-K026 • Center for Substance Abuse Treatment • SAMHSA: 202171 • Public Welfare Foundation • Special Thanks to: • Ed Banks, Ph.D. • Ken Robertson
What affects recidivism?The good, the bad, and the ugly! Understand Risk Understand What Affects Recidivism
67% • Reducing Recidivism:The RNR Framework • Target individual risk • Target needs that are amendable to change • Offer quality programs • Engage offenders in change process
Risk is the likelihood that an offender will engage in future criminal behavior (recidivate). • Risk does NOT refer to dangerousness or likelihood of violence • Static Risk Factors have a demonstrated correlation with criminal behavior • Historical – based on criminal history • Cannot be decreased by intervention What is Risk?
CJ Risk Matters…(3 year, all offenses) Risk is static factors: history of arrests, age of onset, history of incarceration, history of escapes, etc. Ainsworth, Crites, Caudy, & Taxman, 2011
Age & Rearrests Langan & Levin, 2002
Gender Matters Ainsworth, et al 2011
Evidence-Based Practices Lead to Better Outcomes • Education (Psycho-Social) • Non-Directive Counseling • Directive Counseling • Motivational Interviewing • Moral Reasoning • Emotional Skills • 12 Step with Curriculum • Cognitive Processing • Cognitive Behavioral(Social Skills, Behavioral Management, etc.) • Therapeutic Communities (TC) • Contingency Management/Token Economies • Intensive Supervision • Boot Camp • Case Management • Incarceration • TASC • DTAP (Diversion to TX, 12 Month Residential) • Treatment with Sanctions (e.g. Break the Cycle, Seamless System, etc.) • Drug Courts • RNR Supervision • In-Prison TC with Aftercare
Better Outcomes via Tx Matching Caudy, et al (2011). Using Data to Examine Outcomes: A review of Kansas Department of Corrections. Fairfax, VA: George Mason University.
12 http://www.gmuace.org/tools/
The RNR Simulation Tool • Provide decision support tools for the field that enhance existing practices • Individual level • Program feedback • System building capability • Program Tool focuses on: • Classifying programs to target specific needs • Rating key program features • Linking to meta-analyses/systematic reviews
Compiled National Database (20,000+) or Develop Your Own Database Base Recidivism Rate Reflect Expected Reductions in Recidivism (from Meta-Analysis) • Risk & Need Information • Destabilizers—performance inhibitors • Programs • Expected outcomes
Offender Individual Risk & Need Factors Program Quality Implementation Correctional Programming Individual Outcomes (Reduced Recidivism) Model to Improve Outcomes: Big Picture Organizational Culture • Current recidivism hovers around 67% • 3 year re-arrest rate • How can we make a dent in this at the system and individual level? Focus of EBP Research Focus of RNR & RNR Simulation Tool
RNR via Andrews & Bonta Andrews & Bonta • Antisocial personality patterns • History of antisocial behavior • Antisocial peers • Antisocial attitudes • Family/marital factors • Employment/educational deficits • Lack of prosocial leisure activities • Substance Abuse Updated research • Responsivity, Recidivism, & Clinical Relevance • Substance dependence vs. abuse • Spectrum of needs can override risk (3+) • Change is a function of problem severity • History of antisocial behavior is risk (cannot be changed) • Recidivism reduction is function of targeting specific needs within programs
Severe Substance Use Disorders • A pattern of harmful use of any substance for mood-altering purposes • Includes 6 or more of the following: • Increased tolerance, withdrawal, increased time spent using, difficulty quitting or cutting back, or continued use despite negative consequences • Not the same as substance abuse • Drug of choice matters Major Criminogenic Needs
Major Criminogenic Needs • Criminal Thinking/Lifestyle • A pattern of thinking that rationalizes and supports criminal behavior • Involvement with criminal lifestyle • Should be assessed using a validated instrument
Treatment to address criminal behavior should be cognitive and/or behavioral based programming that has been shown to effectively reduce recidivism. • Deliver controls and treatment in a manner that is consistent with individuals’ learning styles • Considers age, gender, culture, intelligence, motivation, etc. • Translate Risk & Need into Program Placement/Case Decisions • Needs trump risk when there is 3+ needs • Destabilizers require more social controls What is Responsivity?
CJ RISK Criminogenic Needs Substance Tolerance for “Hard Drugs” 3+ Criminal Lifestyle—attitudes, family, peers, personality, substance abuse Stabilizers Supportive Family Stable Employment Education > HS Diploma Stable Housing Location in non-Hot Spots Destabilizers Alcohol Abuse Drug Abuse Family Dysfunction Poor Mental Health Status Employment-Related Issues Literacy Related Problems Housing Instability Location in Hot Spots Gender & Age
What Information do I Need? • Static Risk • From a validated risk assessment tool • Based on criminal history • Demographics • Age and gender • Criminogenic Needs • Substance Use • Criminal thinking/lifestyle • Stabilizers and Destabilizers • Clinically-relevant factors
The RNR Program Tool for Adults Define target behaviors that drive program classification Understand program group classification system
Program Groups Risk Type of Need Type of Stabilizers • Six program groups based on specific target behaviors
Program Groups for SUD Treatment • Offenders with SUDs have unique Tx needs • Program Group A: Addicts • Program Group C: Abusers with Lifestyle Factors • Operationalized essential features • Program content, dosage, implementation fidelity • Example: Group A – most intensive • Individual profile: all CJ risk levels; dependence on hard drugs; multiple criminogenic needs and destabilizers • Program profile: cognitive restructuring techniques; adequate dosage to address high SUD need; clinical staff; evidence-based curricula; medication-assisted treatment
Principles of Effective Interventions • Rehabilitative efforts have a greater impact on recidivism • There is no magic program • There is no one program or program type identified that will consistently have a large impact on recidivism • We do know something about common features of effective correctional practice • What really works? McGuire, 2002; Lipsey & Cullen, 2007
Program Quality Matters • Most programs score < 50% (unsatisfactory) • Program quality (Implementation, Risk-Need Assessment, Orientation) related to Recidivism Lowenkamp, Latessa, & Smith, 2006; see also Nesovic, 2003
Program Tool Factors • Target Population • Program Goals • Program Theory • Client Level Factors • Spectrum of Needs/Severity of Program Needs • Developmental Factors (e.g., age, gender, cognitive, physical) • Program Structure • Program Dosage (a lot unknown, clinical literature) • Implementation Issues • Staffing • Fidelity Monitoring, Training • Quality Assurance
Key Items: Use of a validated risk assessment and focus on appropriate risk levels • Justification: • Use of a validated risk assessment is associated with more effective programs • (Smith, Gendreau, Swartz, 2008) • Provide more intensive services to higher risk individuals • (Lowenkamp, Latessa, and Holsinger, 2006; Andrews & Dowden, 2006)
Key Items: Program focuses on a primary target; uses appropriate content based on the target • Justification: • Focus on criminogenic needs • (Andrews, Bonta, and Hoge, 1990) • Focus on stabilizers and destabilizers • (Ward & Stewart, 2003) • Treatment is theoretically linked to changes in the target • (Cordray & Pion, 2006)
Key Items: Program content with better evidence, use of rewards and sanctions, and addresses specific responsivity factors; • Focus is on treatment matching • Justification: • Programs more effective if consistent with an individual’s learning style • Andrews, Zinger, et al., 1990a; Smith et al., 2009; Taxman, & Marlowe, Douglas, 2006 • Treatment matching improves outcomes • Mee-Lee, Shulman, Fishman, Gastfriend, & Griffith, 2001; Thornton, Gottheil, Weinstein & Kerachsky, 1998; Gastfriend & McLellan, 1997; Barbor, 2008
Key Items: completion criteria, appropriate administration based on target, appropriate staff credentials based on target, staff communication, program evaluation, use of a treatment manual, coaching, technical assistance, quality assurance protocols • Justification: • Implementation fidelity related to effectiveness • Landenberger & Lipsey, 2005; Andrews & Dowden, 2005; McGrew, Bond, Dietzen & Salyers, 1994; Stanard, 1999; Simons, Padesky, Montemarano, Lewis, Murakami, Lamb et al., 2010; Taxman & Bouffard, 2000; Fletcher, et al., 2009; Taxman & Belenko, 2012
Key Items: appropriate clinical hours, sufficient duration based on target, sufficient intensity based on target, sufficient frequency based on target, phases, and aftercare • Justification: • Dosage positively related to effect size • (Landenberger & Lipsey, 2005) • High risk approximately 300 hours of CBT • (Bourgon & Armstrong) • Higher risk saw recidivism reduction with more dosage in drug treatment • (Taxman, Byrne, & Thanner, 2002; Lowenkamp & Latessa, 2005)
Key Items: Social controls in programs are also useful to enhance the impact of the content and dosage of programs • Justification: • Increasing social controls for higher risk individuals can improve outcomes • (Drake, Aos, & Miller, 2009; Padgett, Bales, and Blomberg, 2006; Pattavina, Tusinski-Miofsky, & Byrne, 2009)
Building a Responsive System Identify Core Principles of Responsivity Identify Key Stakeholders
Core Principles of Responsivity • Individual • Match programming and controls to risk and need • Involve the offender in the assessment of risk-need information & selection of options • Focus on motivation to change • Provide feedback reports to offenders on progress • System • Focus on correctional culture to increase receptiveness to treatment • Measure client outcomes to gauge performance and share with partner agencies • Increase communication and build systems of care
What does a “Responsive Jurisdiction” look like? • Screening and assessment • Identify risk and primary criminogenic needs • Link assessment info to specific case plans • Treatment matching • High-quality, evidence-based programming • Sound implementation • Enough dosage to make change • Capacity to address population needs • Alignment between needs and services • Collaboration between CJ and Tx
Identifying Key Stakeholders • Judges • Prosecutors • Defense Attorneys • Probation/Parole Officers • Program Directors/Administrators and Treatment Staff
Jurisdiction Capacity Limitations • CJ agencies often lack capacity for responsivity. • Lack of information within correctional agencies about the specific nature and availability of community-based programs. • Lack of quality decision-support tools to help them assess both individual-level and system capacity issues
Group A Group B Group C Group D Group E Group F
Thank you!!www.gmuace.org/tools This project received funding from Bureau of Justice Assistance, Center for Substance Abuse Treatment, and Public Welfare Foundation. Views expressed here are ours and not the positions or policies of the funders.