Download
1 / 52
580 likes | 2.74k Vues
This document delves into the early history and development of blood group systems, highlighting key milestones from Harvey's theory of circulation in 1628 to Landsteiner's discovery of the ABO blood groups in 1901, which earned him the Nobel Prize in 1930. It examines the classic nine blood group systems and the expansion of knowledge regarding various antigens and their genetic underpinnings. The text also discusses the implications of blood group classification on transfusion medicine and infectious diseases, focusing on the mechanisms of antigen expression and compatibility.

E N D
BLOOD GROUPS Meral Sonmezoglu, MD. Assoc Professor of InfectiousDıseases
Early History of Transfusion • Harvey’s theory of circulation, 1628 • Physick, Philadelphia, 1795 • Blundell, England, 1818 • Problems of sterility, coagulability, intravenous routes ignored
Karl Landsteiner (1868-1943) • Discovered ABO blood groups, 1901 • Nobel Prize, 1930
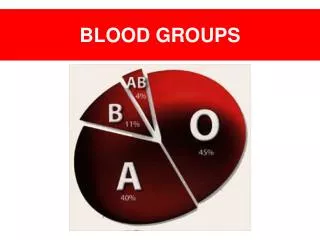
Classic Nine Blood Group Systems • ABO, 1901 • MN and P, 1927 • Rh, 1940 • Lutheran, 1945 • Kell, 1946 • Lewis, 1946 • Duffy, 1950 • Kidd, 1951
All antigens fall into one of fourclassifications: 1. systems 2. collections 3. low incidence antigens (700 series) 4. high incidence antigens (901 series
030 RHAG Duclos Ola DSLK RHAG4 031 FORS FORS1 032 JR Jra 033 LAN Lan
Developments 1951 to mid-1970s • Polymorphisms • Inter-relationships discovered • New systems added to “classic nine” • Diego; Cartwright; Xg; Scianna; Dombrock; Colton; LW; Chido/Rodgers; Hh; Kx; Gerbich; Cromer; Knops; Indian • Antigens added to Rh system • Antigen added to MN system • Monoclonal antibodies to develop better reagents • New techniques, including DNA libraries using RFLPs
Blood Group System • Antigens produced by alleles at single genetic locus, or • Antigens produced by alleles at loci so closely linked that crossing-over never/rarely occurs • Alternative genes: alleles • Antigens: antithetical to each other
Blood Group Collection • Group of antigens that display phenotypic association to each other, without definite genetic independence of all other systems
Blood Group Antigens • 250 antigens, most assigned to one of 33 blood group systems • Approximately 50 antigens not yet assigned, categorized within “collections” (200 series) • Low incidence antigens (700 series) and high incidence antigens (901 series)
RBC Antigens: Associated Functions • Membrane integrity (Kx, Rhnull, Diego) • Transport protein (Kidd) • Adhesion protein (Indian) • Complement regulator/inactivator • (Chido/Rodgers, Cromer, Knops) • Extracellular enzyme (Kell, Yta) • Receptor adhesion (Duffy) • Infectious disease (P globoside, Wrb)
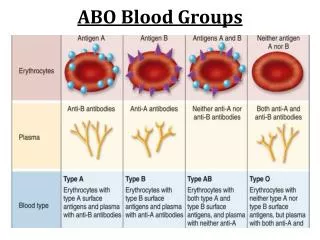
Carbohydrate-based Blood Groups and Collections • Genes control expression of an enzyme that attaches the immunodominant sugar to a precursor backbone on the RBC membrane • ABO • Ii Collection • Lewis • P • Globoside Collection
ABO System • H antigen: H substance is the precursor molecule; fucose bound to subterminal sugar of the oligosaccharide chain • Fucosyltransferase gene for H: chromosome 19 • Subgroups of A and B exist; A subgroups more common
H Antigen • The H gene codes for an enzyme that adds the sugar fucose to the terminal sugar of a precursor substance (PS) • The precursor substance (proteins and lipids) is formed on an oligosaccharide chain (the basic structure)
RBC Precursor Structure RBC Glucose Galactose Precursor Substance (stays the same) N-acetylglucosamine Galactose
Formation of the H antigen RBC Glucose H antigen Galactose N-acetylglucosamine Galactose Fucose
ABO System (2) • A antigen: terminal sugar N-acetylgalactosamine • B antigen: terminal sugar galactose • No O antigen: O gene produces nonfunctional transferase with absence of both A and B • Glycosyltransferase genes: chromosome 9
ABO System (3) • Anti-A and anti-B: naturally occurring, clinically significant; can cause hemolytic transfusion reactions (HTR) and hemolytic disease of the newborn (HDN) • Bombay: normal A and B genes, lack functional H gene, cannot produce H substance, lack A and B antigens, phenotype as group O • Bombay individuals (Oh) have potent anti-H reacting with all RBCs; need rare-donor Bombay RBCs
Ii Blood Group Collection • Same oligosaccharide chains as the A, B, and H antigens, but the interior portion • i antigen, unbranched, on neonatal cells • I antigen, branched, forms during first 2 years of life • Auto-anti-I: mycoplasma infection • Auto-anti-i: Epstein-Barr virus infection
Lewis System • Soluble plasma antigens, adsorbed reversibly onto RBCs • Transfused RBCs assume Lewis phenotype of recipient • Anti-Lea: most are insignificant; never cause HDN • Anti-Leb: insignificant
P Blood Group System • Single antigen, P1 • Individuals lacking P1 antigen are P2 phenotype • Anti-P1 naturally occurring, IgM, usually insignificant
Globoside Blood Group Collection • Pk and P antigens • P is high incidence antigen • Pk antigen is rare • Anti-P: significant IgM, naturally occurring, can cause both HTR and HDN • Donath-Landsteiner antibody is IgG auto-anti-P, biphasic, causing paroxysmal cold hemoglobinuria (PCH)
Polypeptide Blood Groups • Protein antigens under direct genetic control • MNS • Rh • Kell • Kidd • Duffy • Lutheran • Others • Chido/Rodgers • Bg • Xga • Diego
MNS Blood Group System • Major antigens are peptides called glycophorins: • Glycophorin A: M, N • Glycophorin B: S, s, and U • Genes for glycophorins A and B closely linked, chromosome 4 • u denotes absence of U, a high incidence Ag • In absence of U, cells are always S-s- • Patients with anti-U require U-negative blood
MNS Blood Group System (2) • Ena is high incidence Ag on glycophorin A • Ena-negative persons lack glycophorin A, with neither M nor N expression • Ena-negative persons with anti-Ena require rare blood, Ena-negative
MNS Blood Group System (3) • Anti-M: frequent, naturally occurring, either IgM or IgG, rarely significant; unless IgG, then can cause HDN • Anti-N: almost always IgM, not significant • If anti-M/N causes agglutination at 37 C, then use antigen-negative blood; otherwise crossmatch-compatible sufficient
MNS Blood Group System (4) • Anti-S and anti-s both cause HTR and HDN • Patients with anti-S/s will need antigen-negative blood • Anti-U and anti-Ena are both IgG and significant; rare antigen-negative blood required
Rh Blood Group System • Rh proteins encoded by two linked genes on chromosome 1: RHD and RHCE, a haplotype unit • Major antigens: D, C, c, E, and e • D: epitope on RhD protein • C,c and E,e: antithetical antigens on RhCE protein • No d antigen exists
Rh Blood Group System (2) • Rh-positive (85%) and Rh-negative (15%) refer to presence or absence of the D antigen • D antigen most immunogenic of all non-ABO antigens • Anti-D can cause HTR and severe HDN • Nomenclature is confusing and complex: • Fisher-Race: Dd, Cc, Ee • Wiener: R=D, r=absence of D; superscripts (numbers and primes) for Cc or Ee, numbers with R, primes with r
Rh Blood Group System (3) • Weak D (Du): D antigen in reduced quantity • Individuals with weak D are Rh-positive • Individuals with weak D do not make D alloantibodies • Partial D: some epitopes of D antigen missing • Individuals may produce alloanti-D • Individuals are considered Rh-positive • Recipients should receive Rh-negative RBCs
Rh Blood Group System (4) • Rhnull: all Rh antigens absent from RBC surface • Mild hemolytic anemia with stomatocytosis and increased osmotic fragility • Two mutations identified: • RhAG gene for Rh-associated glycoprotein, required for stability/localization of the Rh proteins • RHCE gene mutation in Rh-negative individuals • Antibodies to Rh antigens: usually IgG, reactive at 37 C, and cause HTR and HDN
Kell Blood Group System • More than 20 antigens • Major antigens: K (Kell) and k (Cellano) • Only the D antigen of Rh system is more immunogenic than K among all non-ABO antigens • Antibodies are clinically significant • Other antithetical pairs: Kpa/Kpb, Jsa/Jsb
Kell Blood Group System (2) • In absence of Kx, called the McLeod syndrome, amount of Kell system antigens on RBCs and granulocytes is significantly reduced • Kell and Kx proteins closely associated, Kx protein needed for Kell stability • McLeod syndrome: shortened RBC survival, chronic granulomatous disease, muscular dystrophy, retinitis pigmentosa
Kell Blood Group System (3) • Kell antibodies: immune-stimulated IgG, significant for HTR and HDN • Anti-K most common immune RBC antibody outside ABO and Rh systems, accounting for 1/3 of alloantibodies
Kidd Blood Group System • Primary antigens: Jka and Jkb, encoded by two codominant alleles • Rare: Jknull [Jk(a-b-)] can make anti-Jk3 • Antibodies are IgG immune stimulated, can cause HTR and HDN • Antibodies notorious for being short-lived, and, non-detected, are associated with delayed HTR
Duffy Blood Group System • Major antigens: Fya and Fyb, on intramembranous RBC membrane glycoprotein • Plasmodium vivax receptor; Fy(a-b-) individuals resistant to P. vivax malaria (60% African Americans) • Antibodies are immune stimulated, clinically significant for HTR and HDN
Example 7 Problem: Causes: Resolution:
Example 6 • if alloantibody – antibody ID techniques • if autoantibody – special procedures (minicold panel, prewarming techniques
References • Rudmann, S. V. (2005). Textbook of Blood Banking and Transfusion Medicine (2nd Ed.). Philadelphia, PA: Elsevier Saunders. • Blaney, K. D. and Howard, P. R. (2000). Basic & Applied Concepts of Immunohematology. St. Louis, MO: Mosby, Inc.
Antibody screening • Important that we can detect immune antibodies in antenatal and patients requiring transfusion • Immune antibodies are IgG and don’t readily cause clumping (agglutination of red cells) • We need to use anti-IgG in our tests - Coombs Test