SWEDEN
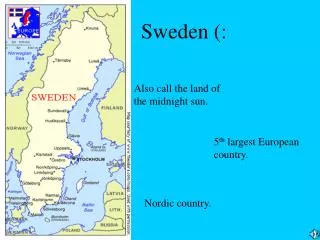
SWEDEN. BACKGROUND. At 450,295 square kilometres (173,860 sq mi), Sweden is the third largest country in the European Union by area


SWEDEN
E N D
Presentation Transcript
BACKGROUND • At 450,295 square kilometres (173,860 sq mi), Sweden is the third largest country in the European Union by area • Sweden has a relatively low population density of 21 inhabitants per square kilometre (54/sq mi) with the population concentrated to the southern half of the country
BACKGROUND • Sweden is an export-oriented mixed economy featuring a modern distribution system, excellent internal and external communications, and a skilled labor force. • Timber, hydropower and iron ore constitute the resource base of an economy heavily oriented toward foreign trade.
HEALTH PROFILE WHO, 2009
HEALTH PROFILE WHO, 2009
HEALTH PROFILE WHO, 2009
HEALTH PROFILE WHO, 2009
SWEDISH SOCIAL CONTEXT • Strong sense of societal solidarity • The care of an elderly is not only a familial but is also a societal concern • Democratic polity • Long period of economic affluence with periods of crises • Long tradition of publicly sponsored health care
ORGANIZATIONAL EVOLUTION Collegium Medicum district MDs- Local Government Crown hospitals; care parishes * Local Boards of Health, Public Health System 1660 1752 1864 1874
ORGANIZATIONAL EVOLUTION Regionalization Prototype welfare state Economic crisis 1958 1960 1970-1980 Present
ORGANIZATION OF HEALTH SYSTEM • The Swedish health-care system is taxpayer-funded and largely decentralized. • Responsibility for health and medical care is shared by the central government, county councils and municipalities. • The Health and Medical Service Act (Hälso- ochsjukvårdslagen, HSL) regulates the responsibilities of the county councils and municipalities.
ORGANIZATION OF HEALTH SYSTEM • The central government establishes principles and guidelines for care to set the political agenda for health and medical care by reaching agreements with the Swedish Association of Local Authorities and Regions (SALAR), which represents the county councils and municipalities.
ORGANIZATIONAL STRUCTURE Structure Function District County Hospitals Inpatient Outpatient services Med, Sx, Rad, Anes 60k-90k Local District Health Services Primary Care, Public Health, MNCHN, School/Industry 2k to 50k
ORGANIZATIONAL STRUCTURE Regional Hospitals Tertiary care Medschool, research 1M Central County Hospitals Specialized wards (500-1,000 beds) and clinics 200k-300k
ORGANIZATIONAL STRUCTURE Structure Function Ministry of Health and Social Affairs National Board of Health and Welfare Planning Rationalization Institute County Councils Federation National Hospitals/Medical Centres Regulation Stewardship/ Planning Policy Evaluation Training Research
National level Federation of Swedish County Councils Parliament Swedish Association of Local Authorities Regional level Government 18 county councils, 2 regions and 1 municipality (regional authority) Ministry of Health and Social Affairs Local level 290 municipalities (local authorities 8 regional hospitals in 6 medical care regions Approx. 20 county hospitals and approx. 40 district county hospitals Special housing and home care for elderly and disabled people Approx. 1100 health centres
Swedish Medical Association/ Professional Organizations • Social Democratic Party • Blue collar unions • White collar unions • Royal Commissions
“Whenever health systems are ranked, Sweden always seems to come top or at the very least a close runner-up” --BBC News, 28 November 2005
HEALTH HUMAN RESOURCE Life Expectancy vs Health Care Spending in 2007 for OECD Countries Source: http://www.oecd.org.
Waiting time to be seen by a physician “The national guarantee of care states that a patient should be able to get an appointment with a primary care physician within 3 days of contacting the clinic. If referred to a dietician by the GP, they should get an appointment within 14 days, and if treatment is deemed necessary by the specialist, it should be given within 10 days.” • http://en.wikipedia.org/wiki/Healthcare_in_Sweden
HEALTH HUMAN RESOURCE • Physicians- interns/residency training, specialist consultants, district physicians, and administrators • Nurses • Pharmacist • Midlevel- physiotherapist, nurse midwives
Factors affecting HR • Distribution to areas and fields of specialties • Supply of doctors • Compensation and work stress • Role of private sectors • Education, training and research opportunities • Cost for the government • Market-reform initiatives were vulnerable to the whims of politicians
According to OECD data, total expenditure on health as a percentage of GDP in Sweden amounted to 8.4% in 1998, slightly less than the EU average of 8.6%. Public health care expenditures amounted to 7.4% of GDP in 1998.
In 1999, approximately 85% (99 billion SEK or 10.9 billion Euros) of total county council net expenditure was spent on health care (excluding dental care and pharmaceuticals), while the remaining 15% was for expenditure on other services, including social welfare, culture and public transportation.
Of the total expenditures of 127 billion SEK spent on health care by the county councils, 99 billion was financed by taxes and not earmarked state grants (78%).
Acute secondary and tertiary health care consumed 62.3% of these revenues, psychiatric care 9.5% and geriatric care 5.8%, while the remainder (22.4%) was spent on primary health care.
National Social Insurance Board • The social insurance system, managed by the National Social Insurance Board, provides financial security in case of sickness and disability. • Insurance is mandatory and covers part of individual income losses due to illness and health care services. • The insurance also covers individual expenditure for prescribed drugs and outpatient care over a high cost-protection limit.
PAYING THE PHYSICIANS The counties employ most physicians on a salaried basis. Incomes are relatively less than in other industrialized nations at about 2x the average personal income.
FINANCING FOR HEALTH CARE FACILITIES Financed largely from country budgets, although the national government makes contribution for special facilities such as university training institutions
SWEDISH HEALTH REGULATION AND GOVERNANCE 1930’s – Legislations passed focusing on maternal and child health low infant mortality rate 1947-1960 – Universal insurance and regionalization of services primary care were provided thru government sickness insurance agency, counties retain hospital services
1960-present – Decentralization health services shifted from central to small counties regional level take full responsibility
Government Type: Democratic Parliament • Ministry of Health and Social Services • National Board of Health and Welfare -- responsible for establishing legal and developmental framework for county implementation of health care -- county is required by central govt to develop 5 yr plans for health care
Health care, health, social issues/ insurance • Dental treatment • eHealth • Elderly care • Health and medical care • Public health • Sickness insurance
The Ministry of Health and Social Affairs is responsible for the whole of the policy The objective of public health policy is to create social conditions to ensure good health on equal terms for the entire population The objective of health and medical care policy is that people must be offered good quality health care that is adapted to needs, accessible and effective
Health System Model “Semashko”