Download
1 / 39
410 likes | 1.41k Vues
Population-based HIV Impact Assessments (PHIA): An Introduction Focusing on Malawi and Zimbabwe. Elizabeth Radin , PhD Technical Specialist – Population-based Surveys Project Director, Malawi & Zimbabwe PHIAs November 6, 2014. Presentation Objectives.

E N D
Population-based HIV Impact Assessments (PHIA): An Introduction Focusing on Malawi and Zimbabwe Elizabeth Radin, PhD Technical Specialist – Population-based Surveys Project Director, Malawi & Zimbabwe PHIAs November 6, 2014
Presentation Objectives • Explain what ICAP’s PHIAs are • Explain why ICAP is doing PHIAs from both a SCIENTIFIC and POLICY perspective • Present how we are approaching the first two PHIAs in Malawi and Zimbabwe • Share information on the future of PHIAs at ICAP
What are ICAP’s PHIAs Population-based HIV Impact Assessment A survey that is: • Nationally-led (MOH, NSO) • In collaboration with CDC • Cross-sectional • Household-based • Nationally and Sub-nationally Representative • Focused on impact-level indicators of the HIV epidemic through biomarkers and self report
What we mean by ‘Impact Assessment’ A Description of Impacts . . . • IMPACT: long term, high-level result (reduced transmission, reduced mortality) OUTCOME: medium-term result (# tested, # on ART) OUTPUT: product of activities (# of health staff trained)
What does a PHIA Assess? • The currents status of the epidemic in a country • The access to and uptake of HIV care and treatment services
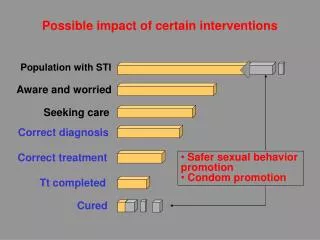
Scientific Rationale for PHIAs Health facilities, and health facility access exists in a spectrum . . . Limited/No Access Pharmacy ART Site Health Center VCT/ANC
Summary: Scientific Rationale • Current data is largely facility-based • Facility-based data describes a subset of the population • It is difficult to infer population measures– such as prevalence or incidence – from facility based data • Population-based surveys are the gold standard for these indicators
Policy Rationale for PHIAs Adults and children with HIV infection receiving ART with PEPFAR support, 2004-2011 4 million Number on ART 2004 2011 El-Sadr WM et al 2012
Policy Rationale for PHIAs After more than a decade of PEPFAR what is that status of the epidemic? For Example: • What is the rate of new infection following prevention efforts? • What is the proportion of Viral Load Suppression following expanded ART coverage?
Sampling for the PHIAs A Two-stage Cluster-based Sampling Strategy: An example: What is the prevalence of coffee drinking at ICAP? Background: ICAP has 1000 staff, 20 Offices, 50 Staff/Office A Census: Ask all 1000 ICAP staff if they drink coffee A Simple Random Sample: Select 10, 100 or 500 ICAP staff and ask if they drink coffee A Cluster-based Sample: Select 5 ICAP country offices, ask all staff in those offices if they drink coffee A Two-stage Cluster-based Sample: Select 10 ICAP country offices, randomly select 25 people from each country office
Sampling for the PHIAs Sampling Strategy: • Using two-stage cluster-based sampling strategy • Sample ~500 Enumeration Areas (EA),stratified by health zone • Sample ~30 Households per EA • Sample size includes ~15,000 HH; ~30,000 individuals • Adults from every HH ~20,000, all children every other HH ~10,000
Similarities between DHS/PHIA • Population-based household survey • Cross-sectional, nationally representative • Household and individual questionnaires • National and subnational HIV prevalence estimates • Household and individual sample size similar
Differences between DHS & PHIA • Biomarkers for CD4 counts, viral load, recency, drug resistance, ARV metabolites, peds • Point-of-Care HIV testing and CD4 testing with return of results • Opportunity to assess global HIV outcomes of interest that are outside domain of DHS • PMTCT • Potential for Treatment as Prevention
ICAP Experience with Pop Surveys • Swaziland HIV Incidence Measurement Survey • Sinazongwe Combination Prevention Evaluation [SCOPE], in partnership with the Zambia MOH • Bukobawithout New Infections, “BukobaBilaMaambukiziMapya,” [BBM2] in Tanzania
Presentation Objective MOH, CDC & ICAP’s Approach to Two PHIAs: Malawi and Zimbabwe
First Two PHIAs: Malawi and Zimbabwe • In collaboration with CDC • Work with Ministries of Health to develop, implement and disseminate findings from PHIA Pilots in Malawi in Zimbabwe • From April 2014-March 2016 • Currently in protocol development and pre-implementation stage
Malawi • 16. 3 Million People • Life expectancy: 54 Years • Causes of Premature Mortality (YLL): HIV/AIDS (23.7%), Malaria (10%), Lower Respiratory Infection (9.7%)1 • HIV Prevalence (age 15-49) • National: 10.3%2 • HIV Care and Treatment: • 675 ART sites, 470,000 patients on ART (83% of need)3 Malawi 2010 DHS. 1 Malawi Global Burden of Disease Study 2010; Institute for Health Metrics and Evaluation (IHME); 2 UNAIDS HIV and AIDS Estimates 3 UNGASS 2013 Malawi Country Progress Report
Zimbabwe • 13 Million People • Life expectancy: 58 Years • Causes of Premature Mortality (YLL): HIV/AIDS (29.0%), Lower respiratory infection (11.7%), Diarrheal disease (6.0%)1 • HIV Care and Treatment: • 665,000 patients on ART • (77% of need)2 DuriKerina et al. HIV/AIDS: The Zimbabwean Situation and Trends. American Journal of Clinical Medicine Research, 2013, Vol. 1, No. 1. 1 Zimbabwe Global Burden of Disease Study 2010; Institute for Health Metrics and Evaluation (IHME); 2 UNGASS 2013 Zimbabwe Country Progress Report
Objectives for Malawi & Zimbabwe PHIAs Primary Objectives: • To estimate HIV incidence (i.e., prevalence of recent HIV infection) in a household-based, nationally representative sample of HIV-infected adults • To estimate the sub-national prevalence of suppressed HIV viral load (<1000 cells/ml3) in a household-based, nationally representative sample of HIV-infected adults
Measuring Incidence Longitudinally Incidence: new infections in a population January 1, 2014 January 1, 2015 - - + - - - - - = .25 cases per person year
Objective 1: Incidence Recent infection (4-6 months) is identified by: Low avidity - weak bonding strength between host antibody and virus. 2) An elevated level of HIV virus in the body . . . And converted into an annualized rate US HIV Incidence (06-09) = .02% Expected Zimbabwe/Malawi Incidence= ~1%
Objective 2: Viral Load Suppression (VLS) Adapted from: aids.gov/federal-resources/policies/care-continuum/
Objectives for Malawi & Zimbabwe PHIAs • To estimate HIV incidence (i.e., prevalence of recent HIV infection) in a household-based, nationally representative sample of HIV-infected adults • To estimate the sub-national prevalence of suppressed HIV viral load (<1000 cells/ml3) in a household-based, nationally representative sample of HIV-infected adults
Objectives for Malawi & Zimbabwe PHIAs Secondary Objectives: • HIV prevalence in adults and children • CD4 T-Cell counts • Transmitted drug resistance • ARV metabolites • Nutrition in HIV positive children • HIV-related risk behaviors • Use of HIV-related services • HIV knowledge and attitudes
Similarities in Malawi and Zimbabwe PHIAs Objectives: • Incidence (national), Viral Load Suppression (zonal) Eligibility Criteria: • Must be a HH member • resides or slept night before in HH • Must give informed consent • All adults in every household • All children (ages 0-14) in every other household
Similarities in Malawi and Zimbabwe PHIAs Survey Procedures: • Collect questionnaire data and blood samples • Carry out POC HIV and CD4 testing • Provide counseling and return results • Refer HIV positives to care • Transport blood samples to central lab for additional testing
Similarities in Malawi and Zimbabwe PHIAs Questionnaires: • Household Questionnaire • Adult Individual Questionnaire • Demographics including marriage • HIV knowledge and attitudes • Reproduction • Sexual history • HIV testing, care and treatment history
Similarities in Malawi and Zimbabwe PHIAs Data Management: • Tablets Cloud server in-country server Laboratory Management: • Central level testing at a national lab (VL, EID, recency) Country Oversight Mechanism: • TWG chaired by MOH • Sub-committees on Management, Protocol, Data, Communications
Unique to Malawi PHIA • Oversampling of high prevalence health zones • for greater precision around cascade analysis • interest in making programmatic assessments/comparisons in future rounds • Sample will include adults aged 15-64
Unique to ZIMPHIA Secondary Objectives: • Prevalence of Syphilis • Describing the extent of stigma Sampling: • Sample will include all adults over 15 Questionnaire: • Module for adolescents aged 10-14
Presentation Objective The Future of PHIAs: The PHIA Project
On the Horizon: ‘the next 20’ In collaboration with CDC and MOHs , ICAP will conduct PHIAs in ~20 sub-Saharan African countries over the next 5 years • No country list yet Focus on building capacity for population-based surveys • Strengthen capacity in epidemiology, surveillance, statistics and national reference laboratory services to collect, analyze, and use morbidity and mortality data
On the Horizon: ‘the next 20’ • Partnerships with experienced groups: • UCSF (KAIS), ICF (DHS), Westat (NHANES), SCHARP (e.g., HPTN/MTN/VTN and SHIMS) and ASLM • Approach for high prevalence countries may differ for low prevalence countries • Use results to assess impact of PEPFAR and guide policies and future programs
Key Messages • ICAP’s PHIAs are Population-based HIV Impact Assessments • Rigorously measure key indicators of the epidemic such as • Incidence • Viral Load Suppression
Key Messages • They will provide information on HIV program effectiveness that can be used to inform future programs and policies • The first two PHIAs will be in Malawi and Zimbabwe • ICAP will work on ~20 PHIAs over the next 5 years
Acknowledgements • The Governments of Malawi & Zimbabwe • United States Centers for Disease Control and Prevention • The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) • Padmaja Patnaik, Suzue Saito, Jessica Justman • The PHIA Team