Simplifying Right Renal Vein Disposition After Laparoscopic Donor Nephrectomy: The VDP Technique
This study evaluates the Venous Disposition Procedure (VDP) for the right renal vein (RRV) in living donor kidney transplants. Conducted between 1998-2010, 60 patients were analyzed, achieving successful transplantation without complications. The VDP technique involves mobilizing the right iliac vein to facilitate an easier end-to-side anastomosis of the RRV. This study demonstrates that the VDP provides a reproducible and efficient solution for dealing with short RRV during laparoscopic nephrectomy, ensuring normal kidney function post-operation with no long-term complications.

Simplifying Right Renal Vein Disposition After Laparoscopic Donor Nephrectomy: The VDP Technique
E N D
Presentation Transcript
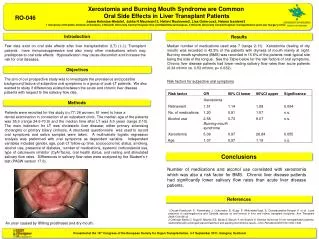
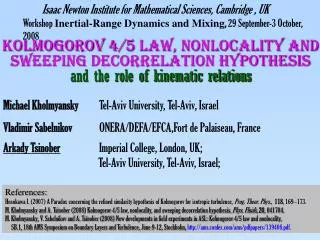
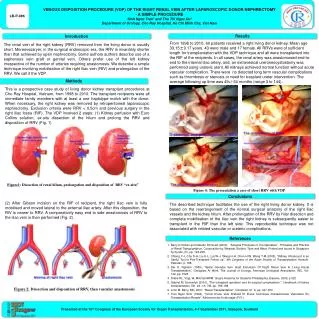
VENOUS DISPOSITION PROCEDURE (VDP) OF THE RIGHT RENAL VEIN AFTER LAPAROSCOPIC DONOR NEPHRECTOMY - A SIMPLE PROCEDURE Sinh Ngoc Tran1 and Thu Thi Ngoc Du1 Department of Urology, Cho Ray Hospital, Ho Chi Minh City, Viet Nam LB-P-086 Replace with logo Introduction Results From 1998 to 2010, 60 patients received a right living donor kidney. Mean age 33.15±9.17 years. 43 were male and 17 female. All RRVs were of sufficient length for transplantation with the VDP technique and all were transplanted into the RIF of the recipients. In all cases, the renal artery was anastomosed end-to-end to the internal iliac artery, and, an extravesical ureroneocystostomy was performed using ureteric stent. All kidneys achieved normal function without acute vascular complication. There were no detected long term vascular complications such as thrombosis or stenosis or need for trasplant ureter intervention. The average following up time was 49+/-34 months (range 3 to 144). The renal vein of the right kidney (RRV) removed from the living donor is usually short. Moreovssaryer, in the surgical endoscopic era, the RRV is invariably shorter than that achieved by open nephrectomy. Some authors authors describe use of a saphenous vein graft or genital vein. Others prefer use of the left kidney irrespective of the number of arteries requiring anastomosis. We describe a simple technique involving mobilisation of the right iliac vein (RIV) and prolongation of the RRV. We call it the VDP. Methods This is a prospective case study of living donor kidney transplant procedures at Cho Ray Hospital, Vietnam, from 1998 to 2010. The transplant recipients were all immediate family members with at least a one haplotype match with the donor. When necessary, the right kidney was removed by retroperitoneal laparoscopic nephrectomy. Exclusion criteria were RRV < 0.5cm and previous surgery in the right iliac fossa (RIF). The VDP involved 2 steps: (1) Kidney perfusion with Euro Collins solution, ex-situ dissection of the hilum and prolong the RRV and disposition of RRV (Fig. 1) Figure1: Dissection of renal hilum, prolongation and disposition of RRV “ex-situ” Figure 4: The presentation a case of short RRV with VDP Conclusions (2) After Gibson incision on the RIF of recipient, the right iliac vein is fully mobilised and moved lateral to the external iliac artery. After this disposition, the RIV is nearer to RRV. A comparatively easy end to side anastomosis of RRV to the iliac vein is then performed (Fig. 2). The described technique facilitates the use of the right living donor kidney. It is based on the rearrangement of the normal surgical anatomy of the right iliac vessels and the kidney hilum. After prolongation of the RRV by hilar disection and complete mobilisation of the iliac vein the right kidney is subsequently easier to transplant in the RIF than the left side. This reproducible technique was not associated with related vascular or ureteric complications. References • Barry D Kahan and Claudio Ponticelli (2000), “Surgical Principles of The Operation”. Principles and Practice of Renal Transplantation, Composition by Wearset, Boldon, Tyne and Wear, Printed and bound in Singapore by Kyodo, (5), pp. 194-208. • Chiang Y-J, Chu S-H, Liu K-L, Lai W-J, Wang H-H, Chen H-W, Wang T-M (2005), “Kidney Ultrasound is an Useful Tool in Pos-Transplant Follow up”, 9th Congress of the Asian Society of Transplantation, Karachi-Pakistan, p. 188. • Dai D. Nghiem (1989), “Spiral Gonadal Vein Graft Extension Of Right Renal Vein In Living Renal Transplantation”, Urologists At Work, The Journal of Urology, American Urological Association, INC, Vol. 142, pp. 1525. • Drake RL, VogL W, Mitchell AWM: Gray's Anatomy for Students Philadelphia, Elsevier, 2005, p 322 • Gabriel M. Danovitch (2010), ”The transplant operation and its surgical complications ”, Handbook of kidney transplantation, 5th ed., ch. VIII, pp. 186-188. • John M. Barry, MD, 2007, “Renal Transplantation”. Campbell, ch. X, pp. 347-350. • Tran Ngoc Sinh (1994), “Choix D’une Voie D’abord Et D’une Technique D’anastomose Vasculaire En Transplantation Renale”. Meùmoire de fin de stage (F.F.I.). Figure 2: Dissection and disposition of RRV, then vascular anastomosis Presented at the 15th Congress of the European Society for Organ Transplantation, 4-7 September 2011, Glasgow, Scotland