Download
1 / 27
330 likes | 479 Vues
Hypokalemia and Hyperkalemia. Dr Madhukar Mittal Medical Endocrinology. Hypokalemia. Spurious Extreme leukocytosis (WBC uptake of K+ in the test tube). Transcellular shift Stress induced catecholamine release Asthma, COPD exacerbation, CHF, MI/Angina, Drug withdrawal syndrome Drugs

E N D
Hypokalemia and Hyperkalemia Dr Madhukar Mittal Medical Endocrinology
Hypokalemia • Spurious • Extreme leukocytosis • (WBC uptake of K+ in the test tube)
Transcellular shift • Stress induced catecholamine release • Asthma, COPD exacerbation, CHF, MI/Angina, Drug withdrawal syndrome • Drugs • Insulin • Theophylline, β2 agonists • Anabolic state • Vit B12 or Folate treatment • GM-CSF • TPN • Hypokalemic periodic paralysis • Decreased Total Body K+
3. Decreased Total Body K+ Renal Loss (urinary K+>20meq/l) Metaboic acidosis Lower GI losses Diarrhea Laxative abuse Metabolic alkalosis Villous adenoma Congenital Cl- losing diarrhea Remote vomiting Remote diuretic use Variable pH Postobstructivediuresis Drugs Aminoglycosides Cisplatin Extra-renal Loss (urinary K+<20meq/l) • Metabolic alkalosis • Mineralocorticoid excess • Primary aldosteronism • Secondary aldosteronism • ↑ mineralocorticoid (Non-aldosterone) action • Normal/↓ BP, No edema, Secondary aldosteronism • Bartter syndrome • Gitelman syndrome • Diuretic abuse • Chronic vomiting • Hypomagnesemia • Metabolic acidosis • DKA • RTA type 1 & 2 • Ureterosigmoidostomy • Amphotericin B • Acetozolamide • Normal pH • Decreased intake • GI losses
Renal Loss (urinary K+>20meq/l) • Metabolic alkalosis • Mineralocorticoid excess • Primary aldosteronism • Secondary aldosteronism • ↑ mineralocorticoid (Non-aldosterone) action • Normal/↓ BP, No edema, Secondary aldosteronism • Bartter syndrome • Gitelman syndrome • Diuretic abuse • Chronic vomiting • Hypomagnesemia • Metabolic acidosis • DKA • RTA type 1 & 2 • Ureterosigmoidostomy • Amphotericin B • Acetozolamide • Normal pH • Decreased intake • GI losses
Extra-renal Loss (urinary K+<20meq/l) • Metaboic acidosis • Lower GI losses • Diarrhea • Laxative abuse • Metabolic alkalosis • Villous adenoma • Congenital Cl- losing diarrhea • Remote vomiting • Remote diuretic use • Variable pH • Postobstructive diuresis • Drugs • Aminoglycosides • Cisplatin
↑Aldosterone, ↓PRA (Primary Aldosteronism) • Adrenal adenoma (Conn syndrome) • Idiopathic hyperplasia • Adrenal carcinoma • Glucocorticoid remediable aldosteronism (GRA)
Hypermineralocorticolism/Aldosteronism(Metabolic alkalosis, Hypokalemia, ↑BP) • ↑↑Aldosterone, ↑PRA (Secondary Aldosteronism) • Edema states (Cirrhosis, CHF, Nephrosis) • Pregnancy (Normal physiologic response) • ↑Renin d/t ↓Renal blood flow • Renal artery stenosis • Accelerated Hypertension (renal vasoconstriction) • Malignant hypertension (arteriolar nephrosclerosis) • Primary reninism • Renin producing tumors • ↓/N BP, No edema • Bartter syndrome • Gitelman syndrome • Chronic vomiting • Diuretic abuse • Hypomagnesemia Hypertensive States
Hypermineralocorticolism/Aldosteronism(Metabolic alkalosis, Hypokalemia, ↑BP) • ↓/N Aldosterone, ↓PRA (↑ Mineralocorticoid action) • Liddle syndrome • Cushing syndrome • AME (apparent mineralocorticoid excess syndrome) • Licorice/Carbenoxolone ingestion • (Glycyrrhizinic acid Ɵ 11-βHSD II enzyme) • CAH – 11βhydroxylase deficiency • DOC (deoxycorticosterone) secreting tumour
Hypermineralocorticolism/Aldosteronism(Metabolic alkalosis, ↓ K+, ↓/N BP) • Bartter syndrome • Hypercalciuria • Gitelman syndrome • ↓Urinary Ca, ↓ serum Mg • Diuretic abuse • Hypomagnesemia • Chronic vomiting • Urine Cl- <10meq/l • Urine Cl- >20meq/l
CVS - ECG • Flattening or inversion of T wave with ST depression • Prominent U waves • Prolonged QT (QU) interval • + prolonged PR interval, wide QRS complex • Atrial and ventricular arrhythmias • Predisposition to digitalis toxicity
Clinical • NeuroMs • Weakness, flaccid paralysis • Cramps, tetany, rhabdomyolysis • Ileus, constipation, urinary retention • Endocrine • Glucose intolerance • Growth retardation, ↓ aldosterone • Renal • ↓ renal blood flow, ↓ GFR • Nephrogenic diabetes insipidus • Increased ammoniagenesis (hepatic encephalopathy) • Chloride wasting/metabolic alkalosis
Treatment • Agent • KCl • Pot bicarbonate and citrate for hypokalemia associated with chronic diarrhea, RTA • Max concentration • <40 mmol/l via peripheral vein • <60 mmol/l via central vein • Infusing solution • NS • Mannitol • Rate of infusion • <20mmol/hr unless paralysis, malignant ventr arrhythmias
Treatment • Montoring • Clinical – NeuroMs • ECG • Plasma K conc. • Hypokalemic periodic paralysis • Ca channel disorder • Oral KCl 0.2-0.4 mmol/Kg every 15-30 min • IV KCL in mannitol • Long term – Actazolamide 125-1000 mg/d, Triamterene 25-100 mg/d, Spironolactone 25-100 mg/d, Dichlorphenamide 50-200 mg/d
Hyperkalemia • Spurious (Pseudo) • Prolonged use of tourniquet • Ischemic blood draws • RBC hemolysis in test tubes • Marked thrombocytosis or leukocytosis
Transcellular shift • Metabolic acidosis • Drugs • Insulin deficiency and hypertonicity • β blockers • Tissue breakdown • Rhabdomyolysis • Tumor lysis syndrome • Intravascular hemolysis • Hyperkalemic periodic paralysis • Drug toxicity • Digitalis • succinylchloline • Chronic Hyperkalemia
3. Chronic Hyperkalemia (Metabolic acidosis, Hypokalemia) • ↓Aldosterone, ↑PRA (Hypoaldosteronism) • Primary adrenal insufficiency • Aldosteronebisynthetic defect • Mutation in aldosteronesynthase gene (cyp 11B2) • CAH – Lipoid, 3β-HSD def, 21-OH-lase deficiency • Heparin • ACE Ɵ, ARBs (selective unresposivensess to angiotensin II) • ↓Aldosterone, ↓PRA (HyporeninemicHypoaldosteronism) • NSAIDS • Chronic TIN, Diabetic Nephropathy, Mild renal failure
3. Chronic Hyperkalemia • ↓Aldosterone, ↓PRA, ↑BP, (Cl- shunt/reabsorption in distal tubule) • PHA-II (Gordon’s syndrome) • Cyclosporine • Distal Type 4 RTA • ↑Aldo, ↑PRA,↓BP (Mineralocorticoid Resistant Hyperkalemia), Impaired distal Na+ reabsorption • PHA-I • Potassium sparing diuretics - Spironolactone, Eplerenone, Triamterene, Amiloride • Trimethoprim • Pentamidine
↓Aldosterone, ↓PRA (Hypoaldosteronism) • NSAIDS • Chronic TIN • Mild renal failure • Cl- shunt/reabsorption in distal tubule (↑BP) • Cyclosporine • Type 4 RTA • Gordon syndrome (PHA-II)
↑Aldosterone, ↑PRA (Mineralocorticoid Resistant Hyperkalemia) • PHA-I • Potassium sparing diuretics • Spironolactone, Eplerenone • Triamterene, Amiloride • Trimethoprim • Pentamidine • ↓BP • Impaired distal Na+ reabsorption
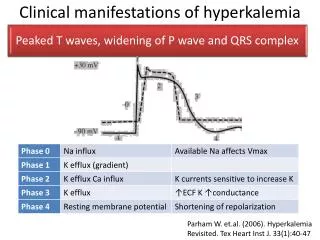
CVS - ECG • Tall peaked (tented) T waves (earliest change) • Short QT interval • Wide QRS, PR interval prolongs → 20 or 30 AV block • ↓ P wave amplitude → complete loss of P waves with associated junctional rhythm • QRS widens → sine wave (ventr. flutter-like) pattern • Eventual asystole
Treatment • Restrict K intake to <40 mmol/day • Stop K supplements • Stop K sparing diuretics
Treatment • Ca gluconate (10%) • 10 ml over 1 -3 min IV • Repeat if no change in ECG after 5-10 min • 10-20 U regular insulin + 25-50g glucose IVI • NaHCO3 3 amp (50-150mmol) in 1L of 5%D • Nebulizedβ2agonist (albuterol 20mg in 4ml NS)
Treatment • Diuretics – furosemide 60-80 mg/day • Resins (sodium polysterenesulfonate) • 25-50g in 100ml of 20% sorbitol • Retention enema 50g in 50ml of 70% sorbitol in 150ml tap water • Dialysis • For patients with renal failure • Severe life-threatening hyperkalemia unresponsive to conservative treatment • Hemodialysis – most rapid and effective way • Peritoneal dialysis – only 15-20% as effective as hemodialysis