Venous thromboembolism / Pulmonary Embolism
Venous thromboembolism / Pulmonary Embolism. Westly Bailey, MD Emory Family Medicine July 2, 2009. Objectives. Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention . VTE Prevalence.

Venous thromboembolism / Pulmonary Embolism
E N D
Presentation Transcript
Venous thromboembolism / Pulmonary Embolism Westly Bailey, MD Emory Family Medicine July 2, 2009
Objectives • Venous Thromboembolism (VTE) Prevalence • Patho-physiology • Risk Factors • Diagnosis • Pulmonary Embolism (PE) • Management of DVT/PE • Prevention
VTE Prevalence • 600,000 VTE’s in U.S. in 1991 (0.2% of the population). • Incidence is increasing. • Significance? • 50% of untreated DVT’s will be complicated by a PE. • 26% of unrecognized pulmonary embolisms are eventually fatal. • P.E. accounts for 16% of all hospital death. • The Worcester DVT Study. Arch Intern Med. 1991;151:933-938.
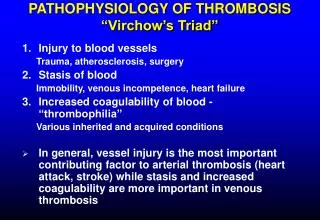
VTE Patho-physiology • Virchow’s Triad • Venous stasis. • Endothelial injury. • Hyper-coagulability. Brotman DJ, Deitcher SR, Lip GY, Matzdorff AC. Virchow's triad revisited. South Med J. 2004;97:213-214.
VTE Patho-physiology • Dislodgement of blood clot • Lower Extremities (65%-90%) • Pelvic venous system • Renal venous system • Upper Extremity • Right Heart http://www.realage.com/health_guides/DVT/img/DVT_art_v1.jpg
VTE Patho-physiology http://www.nursinglink.com/nfs/nursinglink/attachment_images/0009/1991/DVT-main_Full.jpg http://clistersbackchannel.files.wordpress.com/2009/03/dvt1.jpg
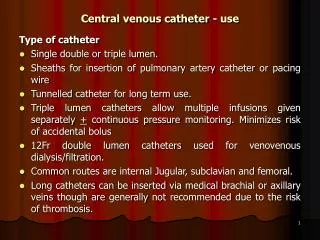
VTE Risk Factors • Pre-existing Conditions • Thrombophilic Disorders • Stroke • Heart Disease • Respiratory Disease • Malignancy • Varicose Veins • Procedures • Central Venous catheter/port/pacemaker.
VTE Risk Factors • History of venous thrombo-embolism • Increasing age (> 60 yrs) • Surgery within prior 3 months or requiring >30mins of anesthesia. • Immobility • Recent travel (within prior 2weeks, >4 hrs).
VTE Risk Factors • Specific to women: • Obesity BMI ≥ 29 • Pregnancy • Hypertension • Heavy smoking (> 25cigs/day) • Hormone replacement therapy • OCP’s 10-30/100,000 users vs. 4-8/100,000 non-users.
Example Scenarios • 38 yr old female presents with pain and mild swelling in L LE. Pt was hiking recently when she slipped, fell and injured R knee. Her knee immediately swelled. She felt unstable w/ walking due to pain and sought care at a local ER. A knee immobilizer was placed. She followed up with an orthopedic doctor who diagnosed an acute ACL rupture. An MRI confirmed this and she underwent allograph repair 3 weeks ago. She is currently doing rehab with a PT.
Example Scenarios • 42 y.o. Caucasian male w/HLD c/o worsening left calf pain which started 3 weeks ago. He exercises at a local gym for 1 hour each day. Lately he has been unable to complete exercise 2/2 calf pain. He notes leg swelling over the past few days as well. • 54 y.o. AAM record producer w/HTN, c/o right calf pain X 2 days. Denies recent illness or change in activities other than several plane trips (>4hrs) over the past month and a road trip (>7 hrs) ~1 wk ago.
Exam Findings http://www.my-varicose-veins.com/images/DVT.jpg http://www.topnews.in/files/dvt.jpg
Anatomy of the Deep Venous System http://www.wsiat.on.ca/images/mlo/medial_veins.jpg
Exam Findings Calf tenderness Homan’s Sign Differential Swelling www.netterimages.com
Well’s Criteria (DVT) • Well’s Criteria (DVT) • Active cancer (tx within <6 mos or palliative care) (1) • Calf swelling (3 cm difference – 10 cm below tib tub) (1) • Collateral superficial veins (1) • Paralysis, paresis, or recent immobilization LE (1) • Pitting edema confined to involved leg (1) • Bedridden within 3 days or surgery w/anesth <3mths (1) • Swollen leg (1) • Alternate diagnosis more likely (-2) Probability: Low (0 pts) Intermediate (1-2) High (3) Lancet 2002;350:1796.
D-Dimer • 96-100% Sensitivity for active VTE if measured by ELISA or immunoturbidimetric method. • Most studies use cutoff <500 ng/mL. • Not highly sensitive if measured by semiquantitative latex agglutination. • A low Well’s Score Criteria plus a normal D-Dimer implies a LOW clinical risk of VTE. • 0.5% of patients develop DVT in 3 months. • Can defer further testing. • What is the risk of DVT in a patient with a moderate or high risk Well’s score and a normal D-Dimer? • Moderate: 3.5% • High risk: 21% Fancher TL, White RH, Kravitz RL. Combined use of rapid D-dimer testing and estimation of clinical probability in the diagnosis of DVT: systematic review. BMJ. 2004;329:821 Ann Fam Med 2007;5:57-62.
Venography • Gold standard • Invasive • Expensive • Primarily a research tool http://www.jaapa.com/Media/Images/48/dximaging1207fig2_47609.jpg
Ultrasonography • Duplex scan of LE • Compressibility of the vein • Doppler flow within the vein • Asymptomatic patient with proximal LE DVT • Sensitivity: 47-62% • Symptomatic patient with proximal LE DVT • Sensitivity: 89-96% • Specificity: 94-99% • Symptomatic patient with distal LE DVT • Sensitivity: 73-93%
A Presenting sign in: Pancreatic cancer Prostate cancer Late sign in: Breast cancer Lung cancer Uterine cancer Brain cancer Pulmonary Embolism
History • History • Dyspnea (73%) • Pleuritic Chest pain (66%) • Cough (37%) • Hemoptysis (13%) • With a large PE: • Syncope • Hypotension Stein, PD, et al. Chest 1991 Sep;100(3):598-603. Stein, PD, et al. Am J Cardiol 1991; 68:1723-
Well’s Criteria ≤2: Low 2 to 6: Moderate >6: High Adapted with permission from Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED d-dimer. Thromb Haemost 2000;83:416-20. Am J Med 2002;113:270
Exam Findings • Fever: T <102 F • Tachypnea (70%) • Rales • Hypoxia • Tachycardia (30%) • S4 • Accentuated pulmonic component of S2 • No leg symptoms
Exam Findings • “Massive PE” • SBP <90 or a drop in baseline SBP by ≥ 40mmHg • Acute right heart failure • Elevated J.V.P. • Right-sided S3 • Parasternal lift
Diagnosis • Labs • Arterial Blood Gas (ABG) • Beta Natriuretic Peptide (BNP) • Cardiac Enzymes: Troponin • D-Dimer • Diagnostic Studies • EKG • Imaging • CXR • Ultrasound • V/Q Scan • Angiography
ABG Findings • Hypoxemia • Hypocapnia (low CO2) • Respiratory Alkalosis • A-a gradient >20 mm Hg • (713(FIO2) – PaCO2/0.8) – PaO2 • Massive PE: hypercapnia, mix resp and metabolic acidosis (inc lactic acid) • Patients with RA pulse ox readings <95% are at increased risk of in-hospital complications, resp failure, cardiogenic shock, death.
BNP • Insensitive test • Not ALL patients with PE have high BNP • Good prognostic value measure: if BNP >90 associated with adverse clinical outcomes (death, CPR, mechanical vent, pressure support, thrombolysis, embolectomy).
Troponin • High in 30-50% of pts with mod to large PE • Prognostic value if combined pro-NT BNP • Trop I >0.07 + NT-proBNP >600 = high 40 day mortality
D-Dimer • High Sensitivity: 95% of PE pts will be positive • Low Specificity • High Negative Predictive Value
RAD Right Atrial Enlargement
EKG Findings • EKG • 2 Most Common finding on EKG: • Nonspecific ST-segment and T-wave changes • Sinus Tachycardia • Historical abnormality suggestive of PE • S1Q3T3 • Right ventricular strain • New incomplete RBBB
Chest X-Ray • Normal • Atelectasis and/or pulmonary parenchymal abnormality • Pleural Effusion • Cardiomegally
Ventilation – Perfusion (VQ) Scan • Results • Indeterminate • Normal • Low probability • Intermediate probability • High probability
Spiral Chest CT • Detection of pulmonary embolism by timed application of contrast to the pulmonary vasculature • Heterogeneity in results across trials. • Sensitivity: 40-100% (PIOPED 2: 83%) • Specificity: 78-100% (PIOPED 2: 96%) Segal J, Eng J, Tamariz L, Bass E. Review of the evidence on diagnosis of deep venous thrombosis and pulmonary embolism. Ann Fam Med. 2007;5:63-73.
Spiral Chest CT www.imagingpathways.health.wa.gov.au/.../vq.jpg
PE Diagnosis • VQ scanning versus Spiral CT Chest • Randomized trial of patients suspected of having PE, n=1471 False Negative Rate Spiral CT 0.6% VQ Scan 1.0%
VTE Diagnosis • What should you do if you have a patient with a high probability Well’s score for PE and a negative spiral CT Chest? • Single or sequential duplex scan of the LE OR • Pulmonary angiography
Pulmonary Angiogram Pulmonary Angiogram • Gold Standard • Not easily accessible • Radiologist dependent • Sensitivity (83%) • Specificity (96%): if negative, very low likelihood that pt has P.E.
Echocardiogram Echocardiogram • Increased Right Ventricle Size • Decreased Right Ventricular Function • Tricuspid Regurgitation Rarely: • RV thrombus • Regional wall motion abnormalities that spare the right ventricle apex (McConnell’s Sign)
Pulmonary embolism severity index (PESI) • Points are assigned as follows: • 1 for each year of age • 10 for male sex • 20 for HR>110 beats/min • 10 for heart failure • 30 for malignancy • 10 for chronic lung disease • 30 for SBP<100 • 20 for RR>30 • 20 for temp <36 degrees Celcius • 60 for AMS • 20 for PaO2<90%
PESI score • Class I <65 • Class II 66-85 • Class III 86-105 • Class IV 106-125 • Class V >125 • 30 day mortality increases with each class • Class V has a 25 fold higher risk of postdischarge death than Class I • The PESI score can help you determine LOS at a hospital
Treatment of DVT • Not Pregnant • Low Molecular Weight Heparin (LMWH) • 1 mg/kg q 12 hrs or 1.5 mg/kg q 24 hrs • Coumadin x 3 months (Goal INR 2-3) • LMWH should be overlapped until both of the following conditions are met: • INR >2 x days • At least five days of LMWH given • Pressure stockings
Treatment of DVT • Pregnant • LMWH • Monitor anti-factor Xa levels q 4 weeks (4 hrs after dose) • Goal: 0.6 – 1.0 IU/ml (bid dosing) or 1-2 IU/ml for q day dosing • Heparin bridge • Stop LMWH 2 weeks before delivery. No epidural within 24 hrs of LWMW. • Start Unfractionated Heparin with goal PTT 1.5-2.3 X normal • Hold for delivery with restart 6 hours after vaginal delivery or 12 hours after C-section. • Coumadin in the post-partum period • Three to Six months • Need to cover at least six weeks post-partum • Ok for breast-feeding.
Treatment of DVT • Obesity: • Enoxaparin – Drop dose by 25% for patients >144 kg • Dalteparin – Drop dose by 25% for patients > 190 kg
Treatment of DVT • Chronic Kidney Disease • No consensus guidelines exist for choice of anticoagulation in patients with GFR < 30 ml/min • Bleeding risk and recurrent VTE risk are higher in such patients. • If using LMWH, consider monitoring anti-factor Xa levels.
Treatment of DVT • Malignancy • LMWH favored over coumadin for longterm therapy • CLOT Trial (Randomized trial,n=672) • Recurrent DVT 8% (dalteparin) vs 16% (warfarin) • No difference in major bleeding, death • Dosing: Dalteparin (Fragmin) 200 IU/kg q day x 1 month, then 150 IU/kg q day x 5 months. • Max dose: 18,000 IU/day • No monitoring required.
Unfractioned Heparin vs LMWH • Meta-analyses have shown: • Lower recurrence DVT (2.7% vs 7.0%) • Lower incidence major bleeding (0.9% vs 3.2%) • Lower death rate at 3 months (OR 0.71 (0.53-0.94)) (All favoring LMWH) Am J Med 1996 Mar;100(3):269-77 Ann Intern Med 1999 May 18;130(10):800-9