Download
1 / 57
650 likes | 1.02k Vues
ANAESTHESIA FOR NEUROIMAGING CECT, MRI, ANGIOGRAPHY. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Guidelines for non-operating room anesthetizing location. Reliable oxygen source with a backup Suction source Waste gas scavenging Minimum mandatory monitoring equipment

E N D
ANAESTHESIA FOR NEUROIMAGINGCECT, MRI, ANGIOGRAPHY www.anaesthesia.co.inanaesthesia.co.in@gmail.com
Guidelines for non-operating room anesthetizing location • Reliable oxygen source with a backup • Suction source • Waste gas scavenging • Minimum mandatory monitoring equipment • Sufficient safe electrical outlets • Patient and anesthesia machine illumination with battery powered backup.
Guidelines for non-operating room anesthetizing location (contd…) • Sufficient space for anesthesia care team. • Emergency cart with defibrillator • Emergency drugs and equipments. • Reliable two-way communication to report assistance
Facilities • Location • Unfamiliar anesthetic equipments • Anesthetic implication of procedure performed • Remoteness of available assistance • Personnel less familiar than usual in operating suites. • Space for anaesthesia equipment and drugs may be limited • Piped gases, suction, isolates a power not always available
Recovery • Medically stable before discharge/ transfer • Recovery facilities and staff • Provision of O2 delivery and monitoring on transport cart • Availability of personnel trained in ACLS • Specific discharge criteria
Radiation safety • Dosimeter • Maximal permissible radiation dose • 50 MSV (milliseverts) annually • life time cumulative dose of 10 msv x age • Monthly exposure of 0.5 MSV for pregnant women • Lead aprons antithyroid shields, using movable leaded glass screens, • Innovative techniques: Video monitoring and remote mirroring of monitor data
Principles of Computed Tomography • Two dimensional, cross sectional image • Typical scan comprises 20 sections • Absorption value Hounsfield unit • Isodense normal brain parenchyma • Hyperdense bone, fresh haemorrhage • Hypodense Edema, Necrosis
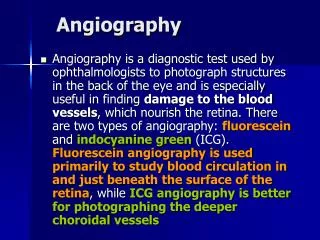
C T Scan (Indications) • Intracranial pathology • Intraspinal and paraspinal pathology • Enhancement of • intracranial neoplasms, • infarcts, • vascular lesions, • abscesses by intravenous administration of water-soluble iodinated contrast material
CT Scan (Indications) contd… • Modality of choice for detection of skull fractures and acute SAH in emergency setting • Spiral acquisition CT scan is also popular because larger anatomic regions can be scanned quickly
CT scan (Limitations) • Insensitive for posterior fossa Structures view as Image degradation by the artifact is produced by interface of bone and brain parenchyma. • Contrast media are to be introduced in GI system in patients who are sedated or anaesthetized.
Anaesthetic Considerations • Risk of aspiration if Airways unprotected • Risk of adverse sequelae associated with contrast media is higher in patient undergoing CECT versus other types of radiological studies
Contrast considerations • Goldberg divided these reactions into five classes • Vasomotor, peripheral vasodilation from direct action of the Intravenous Contrast Medium • Vasovagal from CNS effects of the media • Dermal, erythematous and urticarial response to histamine release • Osmotic • Anaphylactoid which involves release of histamine and other mediators
Prevention of Contrast reactions • Fluid administration • Before, during, and after procedure • Low osmolality contrast media • Acetyl cysteine
Anesthetic Considerations • IV Sedation/General Anesthesia is required to: • reduce patient movement • children/mentally challenged/confused • provide airway protection • unconscious • provide controlled ventilation • reduce anxiety and claustrophobia
Principles of MRI • Atomic nuclei with odd number of protons or neutrons. • H1, C13, F19, Na23, P31 • Biological tissues have high water content. • H+ acts as Dipole • Magnetic Dipole movement • Gyromagnetic property
Magnetic resonance imaging • Anaesthesia in the MRI suite poses unique problems • Limited patient access and visibility • Absolute need to exclude ferromagnetic components • Magnetic field interference /malfunction of monitoring equipment • Nil movement of anesthetic and monitoring equipments • Limited access to emergency personnel
Fig. 1A. —Photographs show aftermath of incident 2, which occurred at first institution. Portable anesthesia tank of nitrous oxide (arrows) lies in bore of 1.5-T MR unit. T = table.
Safety considerations • Effect of magnet or ferrous objects- dislodgement and malfunction of implanted biologic devices • Vascular clips, shunts, wired spiral ET parameter, ICD, mechanical heart values, implanted biological pumps
Safety considerations (Contd…) • Problems with ICD’s and cardiac pacemaker include • Heating by induced current • Inhibition of pacemaker output • Reed switch malfunctioning • Torque on pacemaker • Death from torque of vascular clip with MRI magnetic field has been reported • Clips with low ferromagnetic properties safe <1.5 Tesla
Anaesthesic considerations • Cerebrovascular disease and CAD • Intracranial mass lesion • Hyperkalemic response: • Upper motor & Lower Motor Leisons • Encephalitis • CVA • Closed head injury • severe burns • Acute trauma • Patients after prolonged bed rest
General considerations (contd…) • Prolonged patient immobility: increased CNS depressant effects of anesthesia. • Inadequate history due to a decreased level of consciousness • Full stomach, cervical spine injury and multiple organ involvement
Location of anaesthetic equipment • Outside the magnetic field (5-30 G) line 8-9 feet from head • Requires long monitor leads ventilation tubings • Large compressive volume in circuit • Delay in changes of volatile gas concentrations • Increased risk of disconnection • Close to magnetic field • Must be non-ferromagnetic substance • Electrical equipment require appropriate fibres • Do not move gas machine once scan has begun
Anaesthetic goals • Maintenance of patient immobility and physiologically stability • Manipulating systemic and regional blood flow • Treating sudden unexpected complications during the procedure
Patient immobility • Images are composed of multiple data acquisitions to give the final image • One scan can take up to 20 minutes • Movement at any point can affect image quality • Movement from original position affects the homogeneity and maximal strength of the field
Assessment • Detailed history and patient evaluation (including neurological) • H/o previous surgery, allergy and contrast reactions • Any neck, back or joint pathology • Advised to continue their usual prescribed medications • In female pregnancy should be ruled out
Premedication Anxiolytic • Patient Anxiety (4% of scans are aborted) • confined space • loud noises (greater than 95 db) • temperature of the magnetic bore • length of procedure • education and counseling • gradual familiarization with enclosed space • prone positioning
Premedication (contd…) • In patients with h/o allergies – steroids and antihistamines • Antihypertensives to be continued in hypertensives
Radiation safety • Radiation safety – direct adverse biologic effect of MRI magnetic field are not believed to exist
Anaesthetic Management • Choice of anesthetic technique • Modalities of management: • Intravenous sedation • General anaesthesia
Goals of sedation • To improve patient comfort • Help allay burning pain associated with injection of dye • Allows rapid decrease in level of sedation for neurological testing
Sedation • Conscious sedation is a medically induced CNS depression in which communication is maintained so that the patient can respond to verbal commands • Deep sedation is defined as “medically induced CNS depression in which patient is essentially unconscious and does not respond to verbal commands • In such a state patient breaths spontaneously however protective reflexes may be lost, maintenance of airway is not assured
Sedation • Spectrum • Light to deep • Conscious sedation – deep sedation (without recognition) • Deep sedation – general anaesthesia
Contraindication to sedation • Increased risk of pulmonary aspiration • Possibility of airway obstruction or respiratory irregularities • Raised ICP- raised PaCO2 could be dangerous • Respiratory centre is desensitized to CO2 • Renal or hepatic dysfunction which alters drug kinetics • Uppredictable drug effect, as sedative may increase restlessness
Characteristics of an Ideal Agent for Intravenous Conscious Sedation Rapid onset (lipid solubility) No pain on injection Short duration Inactive metabolites Minimal Cardiopulmonary depression Wide therapeutic index Specific antagonist available
PROPOFOL • Ultra-short acting • Fast onset and short duration of action, antiemetic effects • Unconsciousness within 1 minute • Loss of protective reflexes, apnea • Intermittent boluses or a continuous infusion of 50 to 150 µg/kg/min. • No analgesic properties • Recovery within 10 to 15 minutes
Ketamine • Excellent analgesia and sedation but not immobility. • No respiratory depression • Best used in sedation for painful procedures • IV Ketamine dose (0.5-2.0mg/kg) • Intramuscular injection (3-4mg/kg) • Increases ICP, best avoided in intracranial pathology • Non-purposeful motion associated with ketamine makes its use in MRI limited
Indications for GA • Immobiliy • Pediatrics • Extreme pain on lying • Ventilator dependency • Claustrophobia
Anaesthetic Considerations • Anaesthetic Induction • outside the magnet easier • ideally all monitors are portable and can be brought into the MRI suite • attention to transport gurney (trolley) (ferromagnetic)
Anaesthetic Considerations • Airway Management • Anaesthetic Techniques • volatile agents (only certain gases may be available) • IV (infusion pumps may pose problem)
Anaesthetic Considerations • either ETT (consider Rae) or LMA (no reinforced ETT) • Limited access to patient/airway
Various choices and combinations advocated include • Neurolept anaesthesia • Droperidol / fentanyl / midazolam • Propofol bolus and infusion • Propofol bolus and opioid infusion • Opioid bolus and infusion