Anterior Abdominal wall defects
Anterior Abdominal wall defects. By Dr Anyanwu Paschal Consultant Paediatric Surgeon National Hospital, Abuja. Anterior abdominal wall defects. What are they? Common types of interest Causes Presentation PathoPhysiology Investigation Treatment of.

Anterior Abdominal wall defects
E N D
Presentation Transcript
Anterior Abdominal wall defects By Dr Anyanwu Paschal Consultant Paediatric Surgeon National Hospital, Abuja.
Anterior abdominal wall defects • What are they? • Common types of interest • Causes • Presentation • PathoPhysiology • Investigation • Treatment of.
What are anterior abdominal wall defects • These are a group of conditions, congenital and acquired in which there is defective formation or loss of integrity of one or more layers of the anterior abdominal wall. • Consequently these defects are either obvious/ present at birth or are noticed over time as the child grow’s. • Some cause minimal physiologic derangement while many more result in severe physiologic derangements if untreated and usually would result in death of the child unattended to. • Also are part of larger series of anomalies constituting some syndromes.
Types of anterior abdominal wall defects • Congenital group. These are those that occur in utero, consequently the children are born with them. They include the following, • Omphalocele • Gastroschisis • Prune Belly syndrome • Bladder extrophy • Acquired group. These result usually in the course of the child’s life, some times there is a precipitating cause. Examples inclue; • Umbilical hernias • Ventral hernias
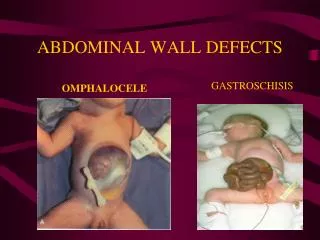
omphalocele • These are congenital conditions in which there complete defect in the development of the entire layers of the anterior abdominal wall usually centered on the location of the umbilicus. • Consequently the intra abdominal viscera to varying degrees are exposed through these defects usually covered by a thin transparent membrane which may or may not be intact. • Usually results from problems with the migration of the lateral mesoderm during development of the anterior abdominal wall. • The size of the defect varies and is usually dictates how much intra abdominal viscera herniates out. The concept of an omphalocele major or minor is based on a defect size greater or less than 5 cm. • More important in the management of these newborn is whether the membrane is intact or ruptured. • Most omphalocele are associated with other congenital anomalies especially cardiac as well as being associated with some syndromes. The pentalogy of Cantrell, the Beckwitt Weidman syndromes, Lower midline syndromes, etc.
Omphalocele continued • Infants with omphalocele are risk of; • Hypothermia, • Hypoglycaemia, • Hypovolaemia, • Other risk are infection, trauma, bowel obstruction, respiratory difficulties. • Initial management of newborn with omphalocele is to correct and prevent the hypovolaemia, hypothermia and hypoglycaemia. Afterwards efforts to provide cover for the exposed viscera is the next course of treatment. • Repairing the defect in omphalocele can be operative or nonoperative. • The operation can be primary or staged/ delayed • Also the operation can be as an emergency or non emergency.
omphalocele • The prognosis of newborn with omphalocele is influenced by the following; • Is the membrane intact or ruptured • What’s the size of the defect • Are there associated anomalies and how severe are these. • It is always important to be able to distinguish and differentiate between omphaloceles and gastroschisis.
Gastroschisis • In this group of anomalies, there is a full thickness defect of the anterior abdominal wall usually to the side of a normally sited umbilicus, most often to the right. • The size of the defect is usually very narrow and as such the exposed viscera mostly consists of the hollow viscera as the solid organs usually cannot pass through the defect. • The exposed viscera usually lack any membrane cover. • Most gastroschisis result from a vascular accident occurring in utero such as intussusception, abnormal vascular involutions. • Most gastroschisis are usually not associated with any other congenital anomalies or syndromes. When anomalies are present, they are usually restricted to the gastrointestinal system. • Presentation is usually that of a newborn delivered with exposed viscera herniating through a narrow defect usually to the right of the umbilicus.
Gastroschisis • These newborn also are at risk from; • Hypovolaemia • Hypo thermia • Hypogycaemia • Infection. • Initial management involves measures aimed at correcting and preventing the conditions. • When the newborn has been resuscitated, the definitive treatment involves emergency surgery/operation. This could be primary repair or use of extraabdominal silos to encourage expansion of the intraabdominal compartment and then fascial closure or repair later. • There is no room for non operative management. • The outcome for patients with gastro schisis is usually very good to excellent.
Differences between omphalocele and gastroschisis Omphalocele Gastroschisis To the side of the midline Not usually associated with other congenital anomalies Not usually part of a syndrome Defect is usually narrow Treatment is only operative Defect lacks any covering membrane • Central defect • Associated with other congenital anomalies • Maybe syndromic • Defect can be very large • Can be managed non operatively • Defect may be covered by a membrane
omphalocele gastroschisis
Prune belly syndrome • Also known as the triad syndrome, or the eagle barrett syndrome. It characterized by abnormal formation and development of the mesodermal layer of the anterior abdominal wall, usually in it’s lower half. • It is also associated with bilateral undescended testes as dilatation of the upper urinary tract. • Usually such affected infants are born with a severely wrinkled looking anterior abdominal wall. • These children are at risk of recurrent urinary and respiratory tract infections as well as failure to thrive or independently ambulate early. • There management involves initial non operative treatment and later series of surgeries to fix the testes and repair the anterior abdominal wall and upper urinary tract if indicated.
Bladder extrophy • In this anomaly, there is failure of development of the entire layer of the lower, midline anterior abdominal wall as well as the anterior bladder wall and pubic symphysis. • Maybe associated with an omphalocele in most cases. • Usually there is associated epispadias of the penis. • Major risk to the child is recurrent urinary tract infection. • Children also develop a waddling gait when the start walking • Treatment involves multiple staged surgeries to repair the bladder, anterior abdominal wall, penis and the bladder neck as well as the pelvic ring.
Acquired anterior abdominal wall defects • Umbilical hernia. • One of the commonest types of hernia found in children especially those of negroid descent. • Usually noticed from the second week of life. • Most of them result from infection at the umbilical stump or from weak umbilical scar due to abnormal collagen. • 85 % of umbilical hernia will resolve spontaneously by 5 to 8 years of age. • Surgery is only indicated in; • Very large hernias, • Those with obstructive symptoms • For cosmetic reasons.
Ventral hernias • Aside the umbilical hernia, these include the epigastric hernias, incisional hernias, paraumbilical hernias.
Neonatal intestinal obstruction By Dr Anyanwu Paschal Consultant Paediatric Surgeon, National Hospital, Abuja.
Neonatal intestinal obstruction • What’s intestinal in the newborn. • What are the common causes • How do they present • Consequence of unrelieved intestinal obstruction in the new born • Investigation • Treatment of newborn intestinal obstruction
Neonatal intestinal obstruction • Neonatal intestinal obstruction is intestinal obstruction occurring the newborn kids between the age of 1 to 28 days of life. • Intestinal obstruction implies a impediment to the normal flow of intestinal luminal content toward the anus. • Intestinal obstruction in the newborn is rather different from all the other age groups because most of the causes of intestinal obstruction in the newborn are congenital rather than acquired causes which is the more usual cause in older age groups. • Also some of the causes of intestinal obstruction in the newborn can be diagnosed before birth during routine antenatal ultrasound screen so as to enable planned delivery of such children in facilities with paediatric surgical services.
Causes • Broadly the causes of intestinal obstruction in the newborn are either in the small intestine also known as upper intestinal obstruction, or in the large intestine also known as lower intestinal obstruction. • Additionally, the causes of the intestinal obstruction maybe mechanical or functional. • Cause of upper intestinal obstruction include; • Malrotation syndrome. • Duodenal atresia • Jejunoileal atresia • Internal hernias • Congenital bands
Causes • Causes of lower intestinal obstruction include the following; • Hirschsprung’s disease • Anorectal malformation • Colonic atresia • Small left colon syndrome • Meconium plug syndrome • Intestinal neuronal dysplasia
Presentation • Antenatal polyhydraminous • Bile stained vomiting • Abdominal distension • Failure to pass meconium • Dehydration • Reduced urinary output • Weakness and reduced activity • shock
Consequence of unresolved intestinal obstruction • Continued fluid and electrolyte loss from vomiting and distension • Fail in the blood supply to the involved bowel • Bacterial overgrowth and translocation across the compromised bowel • Septicaemia • Hypovolaemic shock • Septic shock • Multiple organ dysfunction.
Investigation of neonatal intestinal obstruction • Plain xray in erect and supine views. • Erect view showing multiple air fluid levels. • May show the double bubble sign of duodenal obstruction • Supine view showing the dilated/ distended bowel loops • May also reveal absence of air in the distal colon. • Abdominal ultrasound scan, especially with doppler may help to diagnose mid gut volvulus and malrotation syndrome. • Contrast xrays, like barium/gastrografin enema
Treatment • Treatment of neonatal intestinal obstruction involves initial resuscitation of the child before definitive treatment dictated by the identified cause of the obstruction. • Resuscitation involves; • Correcting all fluid and electrolyte derangements • Nasogastric tube to decompress a dilated stomach • Urethral catheterization to monitor adequacy of the fluid resuscitation • Antibiotics to control sepsis.
Definitive treatment • Definitive treatment is usually dictated by the identified pathology. • Most cases would require surgery to address the offending pathology. • 1, malrotation syndrome; • Exploratory laparotomy, • Release of any volvulus ( detorsion) • Release of Ladd’s bands • Appendectomy • Widen the mesenteric base. • The above is also know as the Ladd’s procedure.
Definitive treatment • Duodenal atresia; • Exploratory laparotomy • Duodenoduodenostomy • Excision of duodenal membrane/web • Jejuno-ileal atresia; • Exploratory laparotomy • Resection of atretic portion and re-establish bowel continuity.
Definitve treatment • Hirschsprung’s disease; • Initially non operative using bowel washout. • May require a colostomy to aid bowel decompression • A pull through surgery by the Swenson, Soave or the Duhamel technique. • Anorectal malformation; • Anoplasty in the newborn period for very low anomalies • Colostomy in the newborn period for all other forms • Posterior sagittal anorectoplasty” PSARP” at 6 months to 1 year of age