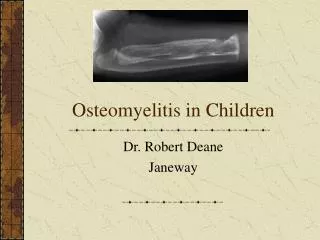
OSTEOMYELITIS
OSTEOMYELITIS. The word “osteomyelitis” originates from the ancient Greek words osteon (bone) and muelinos (marrow) Osteomyelitis is an inflammation of bone & bone marrow. Osteomyelitis is an inflammatory condition of bone begins as an infection of the

OSTEOMYELITIS
E N D
Presentation Transcript
The word “osteomyelitis” originates from the ancient Greek words osteon (bone) and muelinos (marrow) • Osteomyelitis is an inflammation of bone & bone marrow
Osteomyelitis is an inflammatory condition of bone begins as an infection of the medullary cavity and haversian systems and extends to involve the periosteum of the affected area.
Suppurative osteomyelitis • Acute suppurative osteomyelitis • Chronic suppurative osteomyelitis • Infantile osteomyelitis • Non suppurative / sclerosing osteomyelitis • Chronic focal sclerosing osteomyelitis(condensing osteitis) - Chronic diffuse sclerosing osteomyelitis - Chronic osteomyelitis with proliferative periostitis (Garrè's chronic non suppurative sclerosingosteitis)
Specific osteomyelitis • 1. Tuberculous osteomyelitis • 2. Syphilitic osteomyelitis • 3. Actinomycotic osteomyelitis
ETIOLOGY • Most frequently extension of periapical infection • Direct penetration - Physical injury such as Wounds, fracture or surgery • Hematogenous • Bloodstream
Pathogenesis • In the maxillofacial region, osteomyelitis primarily occurs as a result of contiguous spread of odontogenic infections or as a result of trauma. • Primary hematogenous osteomyelitis is rare in the maxillofacial region, generally occurring in the very young. • The adult process is initiated by an inoculation of bacteria into the jawbones. This can occur with the extraction of teeth, root canal therapy, or fractures of the maxilla or mandible. • This initial insult results in a bacteria-induced inflammatory process
PRE DISPOSING FACTORS • Host resistance (Osteomyelitis has been associated with multiple systemic diseases including diabetes, autoimmune states, malignancies, malnutrition, and acquired immunodeficiency syndrome.) • Virulence of micro organism • Jaw vascularity
Conditions altering the Jaw vascularity Radiation Osteoporosis Paget’s disease Fibrous dysplasia Bone malignancy Bone necrosis caused by - mercury, bismath arsenic
ORGANISM INVOLVED Nonspecific oseomyelitis Staphylococcus aureus Staphylococcus albus Streptococcus viridans Anerobes such as bacterioids, porphyromonas or prevotella Specific osteomyelitis may be caused by Mycobacterium tuberculosis Actinomyces organisms treponema palidum etc.
Trauma / infection Ischemia & infiltration of microorganism Acute inflammation Liberation of proteolytic enzyme & destruction Tissue necrosis Vascular thrombosis Necrotic tissue + dead bacteria with WBC’s Pus accumalation Increased intramedullary pressure Vascular collapse Venous stasis & Ischemia.& Pus spread through haversian & nutrient canals Subperiosteal abscess
Further in vascular supply compression of neurovascular bundle OML mediated Mandibular anesthesia Penetration of periosteum Mucosal & Cuteneous Abscess & sinus formation Improvt in host defense + AB therapy =Process become chronic Inflammn+formn of granulation tissue+new bl .Vs formation=lysis of bone Formation of sequestra Involucrum CLOACAE through which pus escapes to ep.surface
Vocabulary Sequestrum: fragment of necrotic bone in the pus Involucrum: Periosteal new bone covering the sequestrum Cloaca: hole in bone during formation of the draining sinus Brodie abscess: reactive bone from periosteum and endosteum which surrounds and contains infection
ACUTE SUPPURATIVE OSTEOMYELITIS • Age – any age group • Site - Involve maxilla or mandible • In maxilla disease remain localized • In mandible more diffuse & wide spread
The incidence of osteomyelitis is much higher in the mandible due to the • dense poorly vascularized cortical plates • single source -the blood supply primarily from the inferior alveolar vessels It is much less common in the maxilla due to • the excellent blood supply from multiple nutrient feeder vessels. • much less dense maxillary bone than the mandible
Presenting signs & symptoms • Deep intense pain • Trismus • High ,intermittent fever • Increased white cell count • Elevated temperature • Regional lymphadenopathy
Parasthesia or anesthesia of lips due involvement of mandibular nerve. • Teeth in affected area are loose & sore causing difficulty in eating • Pus discharge from gingival margin • When periostitis develop, swelling and redness of skin develops
Radiographic features • Acute osteomyelitis do not present significant radiographic changes due to rapidity of process • After 1-2 weeks diffuse lytic changes develop • Trabeculae become fuzzy& indistinct • Gradually radiolucency develop with ill defined margins & having moth – eaten appearance
Investigations • Culture & sensitivity • Imaging Radiographs CT Scan Scintigraphy
Histopathology • Inflammatory changes in medullary spaces with inflammatory edema & infiltration of mainly PMNLs & occasional lymphocytes and plasma cells • Osteoblastic lining of bony trabeculae is lost • Bone may become non viable & begin to resorb
Inflammatory changes in medullary spaces Irregular bony margin Indicating oseoclastic resorption Dead bone with empty lacunae and Absence of osteoblastic lining
Treatment • Debridement • Drainage • Antimicrobial therapy • Complications • Periostitis • Soft tissue abscess • Cellulitis • Pathologic fracture
CHRONIC SUPPURATIVE OSTEOMYELITIS • May develop as a sequelae of periapical infection or in case of inadequate treatment of acute osteomyelitis. • Clinical features are same as acute osteomyelitis, but milder symptoms • Mild pain, increase in temp. slight elevation of leukocyte count. • Teeth may be loose or sore, but not to the extent of interfering with food intake.
Acute exacerbation can lead to acute suppurative osteomyelitis • Bone & overlying skin may be perforated with pus discharge
Chronic Focal Sclerosing Oteomyelitis/ Condensing osteitis • Is an unusual reaction of bone • to mild bacterial infection entering bone through carious tooth • in a person with high degree of tissue resistance & tissue reactivity • Infection behave as a stimulant rather than irritant & Bone reacts with proliferation rather than destruction
Clinical features • Common in children & young adults • Common tooth involved is mandibular first molar with large carious lesion • No signs or symptoms • Mild pain may be present
Radiographic features • IOPA shows well circumscribed radiopaque mass in the periapical region • Entire root out line can be visible with intact lamina dura • Perio. Lig. Will be widened • Sclerotic bone may blend in to adjacent normal bone or may have a distinct border
Radiographic D/D • Benign cemento blastoma • Attached to root and complete root out line is not seen • Surrounded by radiolucent border
Histopathology • Dense mass of bony trabeculae with little interstitial marrow tissue • Many reversal & resting lines in the bone giving pagetoid appearance • Empty osteolytic lacunae • If interstitial marrow tissue is present, will be fibrotic and infiltrated with lymphocytes
Dense mass of bony trabeculae reversal & resting lines Empty lacunae
Treatment • Associated tooth should be extracted or endodontically treated • Sclerotic bone need not be removed unless symptomatic
Chronic Diffuse Sclerosing Oteomyelitis • This condition is similar to focal sclerosing osteomyelitis, but more diffuse
Clinical features • Occur at any age, but common in older persons • No gender predilection • Common in edentulous areas • No significant symptoms • Acute exacerbation may lead to vague pain, unpleasant taste, mild suppuration and some times spontaneous fistula formation and drainage of pus
R/F • Diffuse patchy sclerosis of bone described as cotton- wool appearance • May be extensive and bilateral • Indistinct border between sclerotic bone and normal bone • D/D – • Paget’s disease of bone • Cemento-osseous dysplasia
Histopathology • Dense irregular trabeculae of bone, some of which are bordered by layer of osteoblasts • Focal areas of osteoclastic activity is seen • Bone shows mosaic pattern indicating repeated resorption & repair • Soft tissue between bony trabeculae is fibrous with proliferating fibroblasts, multiple capillaries, and infl. Cells. • In some cases infl. Component is ‘burned out’ leaving only sclerotic bone & fibrosis
D/D • Sclerotic cemental mass • Florid osseous dysplasia
Treatment • Eliminate adjacent foci of chronic infection • Later sclerotic bone may get remodeled or remain sclerotic • Since affected bone is hypovascular & sensitive to inflammatory changes care should be taken to avoid future infections
CHRONIC OSTEOMYELITIS WITH PROLIFERATIVE PERIOSTEITISORGARRE’S OSTEOMYELITISORPERIOSTEITIS OSSIFICANS
It is a distinct type of chronic osteomyelitis characterized by focal gross thickening of periosteum with peripheral reactive bone formation, presenting with typical onion skin like reduplication of cortical plates, resulting from mild infection or irritation.
Etiopathogenesis • Dental caries with associated periapical inflammation • Secondary to • periodontitis, • fracture, • non odontogenic infections i.e.. overlying soft tissue infection or cellulitis.
Mild inflammation act as stimulant & affected periosteum forms several rows of reactive vital bone that are parallel to each other & cause expansion of surface
Clinical features • Age – young below 25 years • Common condition affecting long bones( tibia) • When involves jaw bone common in mandible, in premolar- molar region. • Hyperplasia involve lower border or buccal cortical plate.( isolated lingual cortical plate involvment is rare) • Maxilla is rarely affected • Unifocal or multiple quadrant involvement