Download
1 / 51
510 likes | 593 Vues
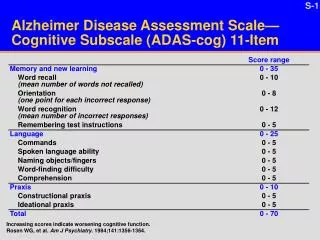
JOURNAL CLUB: Cognitive Function at 3 Years of Age after Fetal Exposure to Antiepileptic Drugs. NEJM 2009; 360(16):1597-1605. 新店耕莘醫院 藥劑部 彭子安 藥師. Introduction.

E N D
JOURNAL CLUB:Cognitive Function at 3 Years of Age after Fetal Exposure to Antiepileptic Drugs NEJM 2009; 360(16):1597-1605 新店耕莘醫院 藥劑部 彭子安 藥師
Introduction • fetal exposure of animals to antiepileptic drugs at doses lower than those that result in structural malformations can produce behavioral and cognitive deficits • the studies of antiepileptic drugs have been lacking to guide the choice of antiepileptic drugs in women who are pregnant or may become pregnant
Aim • performed a cohort study to assess the neurodevelopmental outcomes of children who were exposed in utero to one of several antiepileptic drugs
Methods • study design: • NEAD study: pregnant women with epilepsy who were taking a single antiepileptic agent between 1999 and 2004,in a prospective, observational, multicenter study in the United States and the United Kingdom • primary analysis: comparison of neurodevelopmental outcomes at the age of 6 years after exposure to different antiepileptic drugs in utero • the report focuses on: planned interim analysis of cognitive outcomes in 309 children at 3 years of age
Methods • participants: • included: pregnant women with epilepsy who were receiving monotherapy : ( carbamazepine, lamotrigine, phenytoin, valproate) • control group of non-exposed children was not included • excluded: other antiepileptic drugs, polytherapy, mothers with IQ scores < 70, syphilis tests (+), HIV (+), progressive cerebral disease, other major disease, exposure to teratogenic agents, poor adherence to antiepileptic-drug use, drug abuse in the previous years, and drug-abuse sequelae
Conclusions • in utero exposure to valproate, as compared with other commonly used antiepileptic drugs, is associated with an increased risk of impaired cognitive function at 3 years of age • this finding supports a recommendation that valproate not be used as a first-choice drug in women of childbearing potential
Strengths and limitations • strengths: • prospective design • blinded cognitive assessments with the use of standardized measures • detailed monitoring of multiple potential confounding factors • limitations: • no control group • observational study (not randomised) • the numbers of children exposed to individual antiepileptic drugs are still small • relatively young age of the children at this planned interim analysis
Strengths and limitations • shortcomings: • the study control many of the most important potential confounding factors, but not for all • only occurrence of more than five convulsions during pregnancy were taken into account • breastfeeding information was not complete
Shortcomings of existing studies • may include: a retrospective or inadequately prospective design, insufficient sample size, recruitment and assessment bias, limited length of follow-up, inadequate descriptions of reported anomalies and of procedures used to identify and classify them, questionable choice of controls, and failure to account for potential confounders Emilio Perucca.Lancet Neurol 2005; 4: 781–86
Cochrane report • Cochrane report 2004 : • → the majority of studies on the developmental effects of antiepileptic drugs were of limited quality and that there was little evidence to inform whether the risk differed with the use of different agents
the literature about teratogenesis of cognitive impairment in the offspring of WWE Epilepsia, 50(5):1237–1246, 2009
What is already known on this topic? • the maternal IQ has an important influence on child IQ (Sattler, 1992) →studies were downgraded if they did not control for maternal IQ • the cognitive risk related to AED exposure was not confined to the first trimester, since risk due to exposure may be present throughout pregnancy (Reinisch et al., 1995)
What is the risk of adverse long-term cognitive outcomes in children born to WWE? • Report of the Quality Standards Subcommittee and Therapeutics and Technology Subcommittee of the American Academy of Neurology and the American Epilepsy Society • Q: Is cognitive outcome reduced in children of WWE who are not exposed to AEDs in utero? • two Class II studies (Holmes et al., 2000; Gaily et al.,2004) observed that cognition is not reduced in children of WWE unexposed to AEDs • counseling of WWE who are contemplating pregnancy should reflect that there is probably no increased risk of reduced cognition in the offspring of WWE not taking AEDs (Level B) Epilepsia, 50(5):1237–1246, 2009
What is the risk of adverse long-term cognitive outcomes in children born to WWE? • Q: Is cognition reduced in children of WWE exposed to AEDs in utero? • AEDs in general: showed reduced cognition : two Class II studies (Koch et al., 1999; Oyen et al., 2007) and one Class III study (Hirano et al., 2004)., showed no reduction :One Class II study (Gaily, 1990) and one Class III study (Wide et al., 2002) • Carbamazepine: two Class II studies (Adab et al., 2004; Gaily et al., 2004) and three Class III studies (Scolnik et al., 1994; Wide et al., 2002; Eriksson et al., 2005) showed CBZ does not increase the risk • Valproate: two Class II studies (Adab et al., 2004; Gaily et al., 2004) showed VPA poses an increased risk of poor cognitive outcomes compared to unexposed controls • Phenytoin: One Class II study (Vanoverloop et al., 1992) and two Class III studies (Scolnik et al., 1994; Wide et al., 2002) showed PHT poses an increased risk for poor cognitive outcomes compared to unexposed controls • Phenobarbital: two Class III cohorts (analyzed separately in a single report) of adult men exposed in utero to PB were found to have reduced cognitive abilities compared to normative populations (Reinisch et al., 1995) Epilepsia, 50(5):1237–1246, 2009
What is the risk of adverse long-term cognitive outcomes in children born to WWE? • Q: Is cognition reduced in children of WWE exposed to AEDs in utero? • decreased cognitive outcome in the offspring of WWE should probably not be attributed to CBZ exposure (Level B) • avoiding VPA in WWE during pregnancy, if possible, should be considered to reduce the risk of poor cognitive outcomes (Level B) • avoiding PHT in WWE during pregnancy, if possible, may be considered to reduce the risk of poor cognitive outcomes (Level C) • avoiding PB in WWE during pregnancy, if possible, may be considered to reduce the risk of poor cognitive outcomes (Level C) Epilepsia, 50(5):1237–1246, 2009
What is the risk of adverse long-term cognitive outcomes in children born to WWE? • Q: Does AED polytherapy exposure during pregnancy pose an increased risk for poor cognitive outcome compared to monotherapy? • three Class II studies (Losche et al.,1994; Koch et al., 1999; Gaily et al.,2004) showed that cognitive outcomes are reduced in children exposed to AED polytherapy compared to monotherapy. Outcome assessments included IQ, verbal IQ, and the Columbia Mental Maturity Scale • monotherapy should be considered in place of polytherapy,if possible,for WWE who take AEDs during pregnancyto reduce the risk of poor cognitive outcomes(Level B) Epilepsia, 50(5):1237–1246, 2009
What is the risk of adverse long-term cognitive outcomes in children born to WWE? • Q: Is exposure to a specific AED in utero associated with poor cognitive outcomes compared to other AEDs? • Valproate: two Class II studies (Adab et al., 2004; Gaily et al., 2004) demonstrated reduced cognitive outcomes in children exposed to VPA during pregnancy compared to children exposed to CBZ. In one of the studies, the risk was also greater than PHT (Adab et al., 2004) • Other AEDs: there was no evidence rated Class III or higher regarding other AEDs • for WWE who are pregnant, avoidance of VPA, if possible, should be considered compared to CBZ to reduce the risk of poor cognitive outcomes (Level B) • for WWE who are pregnant, avoidance of VPA, if possible, may be considered compared to PHT to reduce the risk of poor cognitive outcomes (Level C) Epilepsia, 50(5):1237–1246, 2009
The longer term outcome of children born to mothers with epilepsy • Objectives: determine the prevalence of cognitive delay and possible associated dysmorphic features in children exposed to antiepileptic drugs (AEDs) in utero • Design:retrospective study of children born to mothers with epilepsy, children aged between 6 months and 16 years born to mothers with epilepsy • Main outcome: structured interviews, hospital records, clinical examination, and psychometric tests (Wechsler) were used to assess exposure and intelligence quotient (IQ), blinded assessment of photographs was used to score children with characteristic dysmorphic features • Results: N Adab et al., J Neurol Neurosurg Psychiatry 2004;75:1575–1583.
The longer term outcome of children born to mothers with epilepsy N Adab et al., J Neurol Neurosurg Psychiatry 2004;75:1575–1583.
The longer term outcome of children born to mothers with epilepsy N Adab et al., J Neurol Neurosurg Psychiatry 2004;75:1575–1583.
The longer term outcome of children born to mothers with epilepsy N Adab et al., J Neurol Neurosurg Psychiatry 2004;75:1575–1583.
Effects of in-utero exposure on intellectual development • In the past few years, however, several reports have focused on prenatal exposure to valproic acid being especially associated with an increased risk of requiring additional educational support and developmental delay, particularly in verbal performance. • Although these reports suffer from possible bias and small sample size, the fact that different investigations point in the same direction is of particular concern. • This is another area where prospective studies are urgently needed. Emilio Perucca.Lancet Neurol 2005; 4: 781–86
What this study adds? • the reduced IQ effect of valproate is dose dependent • the woman with epilepsy who take valproate, the maternal IQ is not related to child IQ
Adequate and correct information to the patient addition evidence-based review
Provide counseling before pregnancy • the vast majority of WWE (women with epilepsy) have uneventful pregnancies and give birth to perfectly normal children • although the use of AEDs (anti-epileptic drugs) during pregnancy is associated with an increased risk for birth defects, these risks have to be balanced against those associated with uncontrolled seizures • AEDs are also generally indicated during pregnancy if there would otherwise be a risk of generalized convulsive seizures J Neurol. 19 January 2009
Provide counseling before pregnancy • counseling of WWE who are pregnant or are contemplating pregnancy should reflect the following: • here is probably no substantially increased risk (>2 times expected) of cesarean delivery for WWE taking AEDs (Level B). However, there is possibly a moderately increased risk (up to 1.5 times expected) of cesarean delivery for WWE taking AEDs (Level C) • there is probably no substantially increased risk (>2 times expected) of late pregnancy bleeding for WWE taking AEDs (Level B) • there is probably no moderately increased risk (>1.5 times expected) of premature contractions or premature labor and delivery for WWE taking AEDs (Level B) • there is possibly a substantially increased risk of premature contractions and premature labor and delivery during pregnancy forWWEwho smoke (Level C)
Provide counseling before pregnancy • seizure freedom for at least 9 months prior to pregnancy is probably associated with a high likelihood (84–92%) of remaining seizure-free during pregnancy (Level B) • although there is evidence that AEDs taken during the first trimester probably increase the risk of MCMs (major congenital malformations) in the offspring of WWE, it cannot be determined if the increased risk is imparted from all AEDs or from only one or some AEDs, therefore, no recommendation is made from this conclusion
Provide counseling before pregnancy • there is a moderately increased risk of birth defects in children with mothers that are treated with AEDs during pregnancy, malformation rates are higher with polytherapy than with monotherapy, and the risk seems to be greater with valproate (VPA) compared with some other AEDs, for valproate, and possibly also other AEDs, the risk increases with the dosage • to reduce the risk of MCMs, avoidance of the use of AED polytherapy during the first trimester of pregnancy, if possible, compared to monotherapy should be considered (Level B) • if possible, avoidance of the use of VPA as part of polytherapy during the first trimester of pregnancy should be considered to decrease the risk of MCMs (Level B) • if possible, avoidance of the use of VPA monotherapy during the first trimester of pregnancy may be considered to decrease the risk of MCMs (Level C) J Neurol. 19 January 2009
Provide counseling before pregnancy • to reduce the risk of MCMs, the use of VPA during the first trimester of pregnancy should be avoided, if possible, compared to the use of carbamazepine (CBZ) (Level A) • to reduce the risk of MCMs, avoidance of the use of polytherapy with VPA during the first trimester of pregnancy, if possible, should be considered, compared to polytherapy without VPA (Level B) • to reduce the risk of MCMs, avoidance of the use of VPA during the first trimester of pregnancy, if possible, may be considered, compared to the use of phenytoin (PHT) or lamotrigine (LTG) (Level C) • limiting the dosage of VPA or LTG during the first trimester, if possible, should be considered to lessen the risk of MCMs (Level B)
Provide counseling before pregnancy • avoidance of the use of VPA, if possible, should be considered to reduce the risk of neural tube defects and facial clefts (Level B) and may be considered to reduce the risk of hypospadias (Level C) • avoidance of PHT, CBZ, and phenobarbital (PB), if possible, may be considered to reduce the risk of specific MCMs: cleft palate for PHT use, posterior cleft palate for CBZ use, and cardiac malformations for PB use (Level C) • most of the major congenital malformations can be detected by ultrasonography J Neurol. 19 January 2009
Provide counseling before pregnancy • higher doses of valproate may be associated with an increased risk of impaired verbal IQ, although this risk needs to be confirmed in appropriate studies • AED-related risks to the fetus could probably be reduced by appropriate treatment adjustments, however, all major changes in treatment should be completed and evaluated before conception • counseling of WWE who are contemplating pregnancy should reflect that there is probably no increased risk of reduced cognition in the offspring of WWE not taking AEDs (Level B) • monotherapy should be considered in place of polytherapy, if possible, for WWE who take AEDs during pregnancy to reduce the risk of poor cognitive outcomes (Level B) • decreased cognitive outcome in the offspring of WWE should probably not be attributed to CBZ exposure (Level B) J Neurol. 19 January 2009
Provide counseling before pregnancy • avoiding VPAin WWE during pregnancy, if possible, should be considered to reduce the risk of poor cognitive outcomes (Level B) • avoiding PHTin WWE during pregnancy, if possible, may be considered to reduce the risk of poor cognitive outcomes (Level C) • avoidingPB in WWE during pregnancy, if possible, may be considered to reduce the risk of poor cognitive outcomes (Level C) • for WWE who are pregnant, avoidance of VPA, if possible, should be considered compared to CBZ to reduce the risk of poor cognitive outcomes (Level B) • for WWE who are pregnant, avoidance of VPA, if possible, may be considered compared to PHT to reduce the risk of poor cognitive outcomes (Level C) J Neurol. 19 January 2009
Provide counseling before pregnancy • pregnancy risk stratification should reflect that the offspring of WWE taking AEDs during pregnancy probably have an increased risk of SGA (small gestational ages) , furthermore, AED use in WWE during pregnancy should be considered in the differential diagnosis of SGA in their offspring (Level B) • pregnancy risk stratification should reflect that neonates born to WWE probably do not have a substantially increased risk of perinatal death (Level B) • pregnancy risk stratification should reflect that the offspring of WWE taking AEDs during pregnancy possibly have an increased risk of 1-minute Apgar scores of <7. Furthermore, AED use in WWE during pregnancy may be considered in the differential diagnosis of a 1-minute Apgar score of <7 in their offspring (Level C)
Provide counseling before pregnancy J Neurol. 19 January 2009 • folate supplementation is recommended from before conception and throughout the first trimester, although we lack evidence for its effectiveness in preventing AED-related teratogenicity • preconceptional folic acid supplementation in WWE may be considered to reduce the risk of MCMs (Level C) • folic acid supplementation is generally recommended to reduce the risk of MCMs during pregnancy (Czeizel et al., 2004), and although the data are insufficient to show that it is effective in WWE, there is no evidence of harm and no reason to suspect that it would not be effective in this group, therefore, the strength of this evidence should not impact the current folic acid supplementation recommendation that all women of childbearing potential, with or without epilepsy, be supplemented with at least 0.4 mg of folic aciddailyprior to conception and during pregnancy (Morbidity and Mortality Weekly Report, 1992), there was insufficient published information to address the dosing of folic acid and whether higher doses offer greater protective benefit to WWE taking AEDs
Provide counseling before pregnancy • pregnancy is unlikely to affect seizure control in those that are seizure-free • AED plasma concentrations frequently decline during pregnancy, plasma concentration monitoring is therefore recommended, and dosage adjustments are often justified in order to maintain seizure control • that phenobarbital, primidone, phenytoin, carbamazepine, levetiracetam, valproate, gabapentin, lamotrigine, oxcarbazepine, and topiramate cross the placenta may be factored into the clinical decision regarding the necessity of AED treatment for a woman with epilepsy (Level B for phenobarbital, primidone, phenytoin, carbamazepine, levetiracetam, and valproate; and Level C for gabapentin, lamotrigine, oxcarbazepine, and topiramate) J Neurol. 19 January 2009
Provide counseling before pregnancy • monitoring of lamotrigine, carbamazepine, and phenytoin levels during pregnancy should be considered (Level B) • monitoring of levetiracetam and oxcarbazepine (as MHD) levels during pregnancy may be considered (Level C) • there is insufficient evidence to support or refute a change in phenobarbital, valproate, primidone, or ethosuximide levels related to pregnancy (Level U), and this lack of evidence should not discourage monitoring levels of these AEDs during pregnancy • the studies reviewed provide some evidence supporting active monitoring of AED levels during pregnancy, this is especially true for lamotrigine where changes in lamotrigine levels were associated with increases in seizure frequency, it seems reasonable to individualize this monitoring for each patient with the aim of maintaining a level near the preconceptional level, presumably at which the woman with epilepsy was doing well with seizure control. however, the studies reviewed fall short of determining that adoption of an active AED-monitoring program would result in improved seizure control during pregnancy
Provide counseling before pregnancy • Unfortunately, the studies reviewed provided no clear data on the timing of the return to the prepregnancy pharmacokinetic state after pregnancy, one study (Pennell et al., 2008) demonstrated that following an empiric postpartum taper schedule of lamotrigine reduced the occurrence of postpartum toxicity, but more systematic information is needed regarding the pharmacokinetic alterations in AED metabolism postpartum for all AEDs in order to determine the management of AED dosing in the postpartum period
reference • Meador KJ, Baker GA, Browning N, et al. Cognitive function at 3 years of age after fetal exposure to antiepileptic drugs. N Engl J Med 2009; 360: 1597–605. • Adab N, Kini U, Vinten J, et al. The longer term outcome of children born to mothers with epilepsy. J Neurol Neurosurg Psychiatry 2004; 75: 1575–83. • Adab N, Tudur SC, Vinten J, Williamson P, Winterbottom J. Common antiepileptic drugs in pregnancy in women with epilepsy. Cochrane Database Syst Rev 2004; 3: CD004848. • Emilio Perucca. Birth defects after prenatal exposure to antiepileptic drugs. Lancet Neurol 2005; 4: 781–86. • E. Gaily, E. Kantola-Sorsa, V. Hiilesmaa, et al. Normal intelligence in children with prenatal exposure to carbamazepine. Neurology 2004;62:28–32. • Torbjo¨rn Tomson , Dina Battino. Pregnancy and epilepsy: what should we tell our patients? J Neurol March 2009 • C. L. Harden, K. J. Meador, P. B. Pennell, et al. Practice Parameter update: Management issues for women with epilepsy—Focus on pregnancy (an evidencebased review): Teratogenesis and perinatal outcomes. Neurology 2009;73;133-141. • C. L. Harden, J. Hopp, T. Y. Ting, et al. Practice Parameter update: Management issues for women withepilepsy—Focus on pregnancy (an evidence-based review): Obstetrical complications and change in seizure frequency. Neurology 2009;73;126-132. • C. L. Harden, Page B. Pennell, Barbara S. Koppel, et al. Management issues for women with epilepsy—Focus on pregnancy (an evidence-based review): III. Vitamin K, folic acid, blood levels, and breast-feeding. Epilepsia, 50(5):1247–1255, 2009.