Download

1 / 59
630 likes | 1.12k Vues
Are We Making a Difference? Time to Put the Patient Experience at the Centre of Clinical Ethics Sue MacRae, RN Bioethicist Joint Centre for Bioethics/ University Health Network. Are We Meeting the Human Needs of Patients?. Evidence

E N D
Are We Making a Difference? Time to Put the Patient Experience at the Centre of Clinical EthicsSue MacRae, RNBioethicistJoint Centre for Bioethics/ University Health Network
Are We Meeting the Human Needs of Patients? • Evidence • Clinical ethics is more than “hot topics”, well publicized and controversial issues • Can we dare to dig a little deeper into the human experience?
Definition of Clinical Ethics • to improve the quality of patient care by identifying, analyzing, and attempting to resolve the ethical problems that arise in the practice of medicine. • starting point for ethical analysis is the encounter between patient and health care provider. • stresses that the process and outcome of patient care is improved by acknowledging and respecting patient’s preferences and values and by empowering patients to make decisions based on their personal health care goals.” Siegler, Pellegrino and Singer,1990
Video excerpts taken from “Through the Patient’s Eyes” Created by: The Picker Institute, Boston www.picker.org
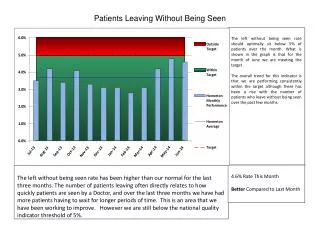
Other data • 10-15% of patients report doctors talk in front of them as if they were not there. • Over 25% of patients report doctors spend less than 5 minutes preparing them for discharge • 40% of dying patients have pain most of the time.
Why? It’s the Right Thing to Do • Reflects values and preferences of those who receive care • Only source of information regarding certain aspects of medical care • Acknowledges “experience” of illness as key
Why? (2) It’s Good Medicine • Acknowledges preferences of patient as valid clinical data • Calibrates the severity of a condition • Forms the basis for defining the condition and severity • Measures treatment complications • Understands how the condition affects patients’ lives • Floyd Fowler, 1995
Why? (3) It Improves Outcomes/Saves money • Treatment choices consistent with choices • Compliance with treatment • Management of chronic illness • Quality of life • Patient and staff satisfaction • Reduces utilization of health care • Reduces cost and complexity
How DO we provide humane, ethical care that matters to patients and their families?
Three Obstacles to Meeting the Needs of Patients • We don’t ground what we do in the needs and experiences of patients • We don’t take care of those that take care • Systems are designed poorly and overly complex
Grounding What We Do In Patient Experience…….. Basic Bioethics
Overcoming the Assumptions and Myths about Patients • Clinically relevant issues are the priority • We do not know what patients need! • Patients have low expectations • Patients can judge quality • Valid and reliable measures exist • Not them, but you.
What Patients Say They Need • Access to care • Respect for patients’ values and preferences • Coordination of care • Information and education • Physical comfort • Emotional support • Involvement of family and friends • Continuity and transition Based on the work of The Picker Institute and Harvard University www.picker.org
Overcoming Assumptions and Myths about Ourselves • Are we using the right model? • Are we asking the right questions? • Are we too focused on the extreme?
The Patient’s Ordeal “Some 13 years later, I realized….I focused largely on the doctor’s practice rather than the patient’s sense of medical crisis, on the rhythms and tempo with which professionals deliver their services rather than on the ordeals the patient’s suffer” William May, 1991
The Clinical Model Decision to Seek Care Information Collection Diagnosis Treatment Rehabilitation Follow-up • 2 slides adapted from work by Dave Gustafson, Ph.D. • University of Madison.
The Human Model Future Self Image Symptoms Providers Feelings Family & Friends Treatment Process Physical Environment
“After all, illness is the experience of disease through an individual patient’s world view and personal circumstance, including the patient’s values and beliefs; emotional, intellectual and financial resources; hopes and dreams. We must consider these values, beliefs, and anxieties as much a part of the patient’s history as is the traditional review of organ systems.” Boumbulian, Day, Delbanco et al, 1991
The Right Questions? Our Perspective • Do we have adequate consent? • Is the patient competent? • Have we identified a substitute decision-maker? • Does the patient have an advance directive? • Are we respecting confidentiality? • Are we telling the truth?
The Right Questions? The Patient Perspective • Do I understand my condition, the treatment alternatives, my future to the extent that I wish? • Am I treated like a human being with dignity and respect? • Who can I trust? What I am going to tell? • Am I being considered as a whole person? • Is my family involved to the extent that I want them to be? • Am I going to have any pain? • Is the healthcare system going to help me cope with my life being turned upside down from illness? • Are my religious/cultural values going to be respected? • Am I going to be abandoned when I die?
Example: Informed Consent • Is the process of informed consent really going to ensure patients understand their condition, treatment alternatives and future to the extent they wish?
Example: Informed Consent • Is the process of informed consent really going to ensure patients understand their condition, treatment alternatives and future to the extent they wish? • What about the research on: • values? • comprehension? • learning styles? • documenting impact of stress on information retention? • on the understanding of complex medical vocabulary? • With people who don’t speak English?
“For every problem, there is one solution that is simple, neat and wrong” Satirist, H.L Mencken
Examples of Initiatives • NEMC • Kaiser Permanente Colorado • Stanford U. School of Medicine • University of Wisconsin • Northwestern Memorial Hospital • University of Worcester
We Don’t Take Care of the People that Take Care • “Asylum” • Clinicians deny their own illness. • To a thoughtful clinician, good clinical practice has always meant both good technical care and good ethical care. • What to do with all that suffering?
“If we were gerbils, we would eat each other.” Staff nurse, UHN Emergency
“At no time in my job does anyone reward me for being a good doctor…….In fact most of what is expected of me, pulls me far away from patients and then I am left in the middle of the night with my own conscience to decide what to do with that. In the end everyone loses.” UHN Senior Physician
“The patient is not just a patient to me, but part of me. I don’t just leave here at the end of the day, like you would if you worked in a regular job, instead day after day I struggle with all the different kinds of cancer that I see in them and in me, and all the different kinds of suffering that we feel together. When they die, I die. Maybe its not a good thing, for either of us, but this is a life of a caregiver.” Nurse, Calgary General Hospital
Systems are Designed Poorly and are Overly Complex • There is no “system” in health care • Supply-side focus • Multiple perspectives • Hierarchies • Waste • Funding forces fragmentation • Perception of higher priorities
“There seemed to be an insistence at Sloan-Kettering, I told them, on the validity of a series of equations that held that, if an individual’s needs exceed what the institution can comfortably provide, then that individual’s needs must therefore be excessive; that whatever level of care the institution is capable of must be adequate, and, therefore, if that care is not good enough, then the patient is unsalvageable.” Evan Handler, Time on Fire
A Contemporary Fable By Donald Ardell
Who Cares About What • Physicians care about: • technical quality of care • good clinical outcomes • appropriate process of care that meets professional standards • cost-effective care? • humane personalized aspects of care? Adapted from slides by Jennifer Daley MD Beth Israel Medical Center, Boston
Who Cares About What (2) • Nurse, therapists about: • excellent process of care that meets current professional standards • humane, personalized care for patients, families and their staff • good clinical outcomes • culture of safety • cost effective care?
Who Cares About What (3) • Health care managers and administrators care about: • cost-effective care • access • service quality • meeting professionally established community standards of clinical practice • staying in business
Who Cares About What (4) • Patients and families care about: • humane, personalized care responsive to their individual needs • retaining, improving, and/or enhancing function and quality of life • access to care • technical competence of physicians and nurses
“Just think about how big the world is - 6 billion people each holding a universe in their own head!” Dirk Koechner, Philosopher