Download
1 / 65
650 likes | 702 Vues
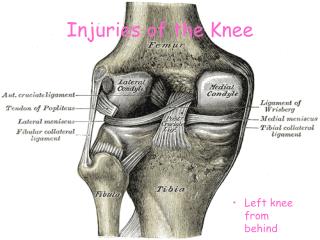
Learn about ACL injuries, MCL tears, patellofemoral pain, ITB syndrome, and more commonly seen knee injuries. Understand indications for surgery, rehabilitation, and factors affecting musculoskeletal health.

E N D
ACL injuries also commonly occur with hyperextension of the knee, deceleration and valgus stress.
INDICATIONS FOR SURGERY: Complete tear; associated meniscal pathology Well motivated person who will do the rehab program; physiologically young Unwilling to change lifestyle; job and sports require twisting, cutting Minimal evidence of DJD
WHEN TO DO SURGERY : Wait at least 3-4 weeks after injury • Decrease the swelling • Decrease Quad inhibition • Decrease hamstring overfiring • Decrease scarring • Increase ROM; decrease stiffness
SURGERIES PERFORMED • Bone-tendon-bone with middle 1/3 of patellar tendon • Semitendinosis and gracilis: fold them in ½ so have a 4 tendon bundle • Allograph: bone-tendon-bone patellar tendon from cadaver • Key in surgery is correct isometric placement of the graph.
80-90% of patients have a good result with surgery going back to previous levels of activity. Some complications that may arise and give a less than favorable result are: • Patellar tendonitis • Patellofemoral pain/chondromalacia • Limited ROM at extremes; loss of even a few degrees of terminal extension is a problem • Stretching out of graph
MCL tears: most common mechanism is a blow to the outside of the knee followed by planting of the foot and twisting of the knee.
There is a high risk of injury to the medial meniscus with MCL tears.
The patella must have balanced muscular forces around it to ride properly in the femoral groove. The VMO should fire before the VL. The VMO/VL ratio should be 1:1 Tight ITB, hamstrings and calf can disrupt muscular balance.
OTHER FACTORS CAUSING PFPS: • Overpronation • Anteversion • Weak Hip ER & ABD • Tibial Varum • Increased Q angle
Complains of pain on knee flexion May complain of snapping Pain gets worse on ROM from full flexion to full extension. Often result of: genu varum; over pronation; femoral anteversion; spinal problems.
Most common area affected is antereomedial shin. Starts out as muscle/tendon injury Can progress to periosteal injury Can end up as a stress fracture
ROM exercises Strengthening Proprioception Agility Running/jumping
Syndesmotic Injury
Over pronation Pes cavus foot Tight calf muscles Tibial varum Anteversion Weak ER of hip
DRUGS USED FOR MUSCULOSKELETAL PATHOLOGY • Analgesics • Drugs that directly affect the healing process • Drugs that do both
NON STEROIDAL ANTIINFLAMMATORY DRUGS (NSAIDS) • Treatment of inflammatory arthritic diseases • Treatment of the “itises”
NSAIDS: SIDE EFFECTS • Gastrointestinal Irritation and Ulceration • Decreased Blood Clotting • Kidney Trouble • Other
Common NSAIDs (OTC) • Bayer (aspirin) • Tylenol (acetaminophen) • Aleve or Naprosyn (naproxen) • Advil (ibuprofen)
Celebrex (celecoxib) Voltaren (diclofenac) Lodine (etodolac) Nalfon (fenoprofen) Indocin (indomethacin) Orudis, Oruvail (ketoprofen) Toradol (ketoralac) Daypro (oxaprozin) Relafen (nabumetone) Clinoril (sulindac) Tolectin (tolmetin) Vioxx (rofecoxib Common NSAIDS (Rx)