Download
1 / 33
330 likes | 563 Vues
Focus on Addressing Cognitive Symptoms. Provided by. In collaboration with. Sponsored by an educational grant from. Program Overview. Part of a 3-component activity for PAs and NPs on achieving sustained remission in MDD Live meetings at AAPA State Chapters and AANP State Organizations

E N D
Focus on Addressing Cognitive Symptoms Provided by In collaboration with Sponsored byan educational grant from
Program Overview Part of a 3-component activity for PAs and NPs on achieving sustained remission in MDD • Live meetings at AAPA State Chapters and AANP State Organizations • Three Clinical Case Challenges posted on myCME.com • Print monograph, a supplement to: • JAAPA • The Clinical Advisor
Content Development Faculty • Cindy Parsons, DNP, PMHNP-BC, FAANP • Staff Assistant • Department of Nursing • University of Tampa • Tampa, FL Charles L. Raison, MD Mary Sue and Mike Shannon Chair for Healthy Minds, Children & Families Professor, School of Human Ecology Professor, Department of Psychiatry School of Medicine and Public Health University of Wisconsin Madison, WI Sattaria S. Dilks, DNP, APRN, FAANP Professor and Co-Coordinator Graduate Program College of Nursing McNeese State University Lake Charles, LA
Learning Objectives At the conclusion of this activity, participants will be better able to: • Assess the impact of acute and residual symptoms of cognitive dysfunction in MDD on patient function, quality of life, risk for relapse, and long-term outcomes • Identify patients who might benefit from new pharmacologic treatment options
Cognitive Symptoms in MDD • Among the core symptom domains included in the diagnostic criteria for a major depressive episode1 • >30% of patients who otherwise respond to antidepressant therapy report residual cognitive symptoms (forgetfulness, inattentiveness, mental slowing, apathy, and word-finding difficulty)2 • Prevalence: • Among all adults with MDD: 30% - 40%1 • Among MDD patients >65 years: 50% - 60%2 1. Poletti S, et al. J Affect Disord. 2014;156:144-149. 2. Fava M, et al. J Clin Psychiatry. 2006;67:1754-1759.
Cognitive Symptoms in MDD (cont’d) • May predate onset of MDD episode • Distinct neurobiology • Heritable • Some deficits may improve with antidepressant therapy • Differences in antidepressant effects on cognition • Often persist after treatment • Impact quality of life and functional outcomes Trivedi M, Greer TL. J Affect Disord. 2014;152:19-27.
4 Key Domains of Cognitive Function in MDD The Diagnostic and Statistical Manual of Mental Disorders (5th ed.;DSM–5; American Psychiatric Association [APA], 2013.
Cognitive Symptoms in Measures of Workplace Performance Cognitive Measures Account for More Variability in Workplace Functioning Than Total Depression Severity N=260; HAM-D17 = Hamilton Depression Scale. McIntyre RS, et al. Compr Psychiatry. 2015;56:279-282.
Decline in Gray Matter Volume in Patients with MDD Compared to Healthy Controls • 3-year prospective study comparing 38 patients with 30 healthy controls • Significant decline in gray matter density was noted in the hippocampus, amygdala, ACC, and DMPFC • Threshold was set at P<.001 Frodl TS, et al. Arch Gen Psychiatry. 2008;65:1156-1165.
Association Between Cognitive Function, Disability, and QoL in Patients Treated for Depression Cognitive dysfunction group had significantly greater impairments on the SDS Conclusion: correlation between objectively measured cognitive dysfunction and poorer patient-reported quality of life and disability Kurlander JL, et al. ECNP 2013. Poster P.1.j.006.
Determinants of Cognitive Symptoms in Depression • Patient’s current age/age at onset • Depression severity at onset • Childhood adversity • Level of educational attainment • Frequency/duration of depressive episodes • MDD subtype • Medical/psychiatric comorbidity • Remission status • Treatment McIntyre RS, et al. Compr Psychiatry. 2015;56:279-282.
Measurement of Cognitive Impairment—Clinical Trials • Domains measured/measurement tools utilized vary across trials • Objective testing: neuropsychologic battery • Mini-Mental State Examination, Montreal Cognitive Assessment not sensitive enough for use in MDD • Subjective tests for clinical use • Perceived Deficits Questionnaire (PDQ) • MGH Cognitive and Physical Functioning Questionnaire (CPFQ) • British Columbia Cognitive Complaint Inventory (BC-CCI)
Consistency of Cognitive Impairment in MDD: Meta-analysis • Significant deficits in executive function, memory, and attention • 700 MDD and 700 control subjects (24 studies) • Significant deficits in executive function and attention • 270 unmedicated MDD and 270 controls (8 studies) “Cognitive impairment represents a core feature of depression that cannot be considered an epiphenomenon that is secondary to mood symptoms…” Rock PL, et al. Psychol Med. 2014;44:2029-2040.
Raising the Bar: Evolving Treatment Goals for MDD Cognitive remission 2014 Improved QoL Functional remission ~2010 Improved function Remission ~2000 Response Symptom reduction Before 1990 QoL = quality of life. McIntyre RS. J Clin Psychiatry. 2013;74:14-18.
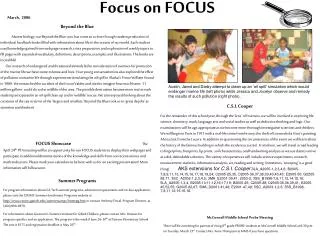
*Percentages are reported as the remaining percent of those with each symptom at baseline that continued to have the symptom at exit. Response was defined as ≥50% reduction in QIDS-SR16. Presence of symptoms was indicated by a QIDS-SR16 domain score ≥1. McClintock SM, et al. J ClinPsychopharmacol. 2011;31:180-186. What Does Failure to Remit Look Like in Those Who Respond to an Antidepressant? Proportion of responders who had symptoms at baseline that persisted at exit* 81.6 Midnocturnal Insomnia 70.8 Sad Mood 70.6 Concentration/Decision-Making 64.6 Energy 63 Restlessness 60.4 Hypersomnia Sleep-Onset Insomnia 57.5 55 General Interest 49 Early-morning Insomnia 38.9 Negative Self-view Slowed Down 35.6 Increased Weight 35.5 31 Decreased Appetite Increased Appetite 27.8 25.1 Decreased Weight 17.1 Suicidal Ideation
MDD-Related Cognitive Dysfunction Tends to Be Persistent • Up to to 50% of individuals with MDD have a suboptimal therapeutic response1 • Among individuals deemed responsive to antidepressant therapy (n=267), cognitive problems, lack of energy, and sleeping difficulties were present for nearly half the time during remissions (39% to 44%) and most of the time (85% to 94%) during depressive episodes over 3 years of follow-up2 1. Baune BT, et al. Psychiatry Res. 2010;176:183-189. 2. Nierenberg AA, et al. Psychol Med. 2010;40:41-50.
Traditional Antidepressants: Effects on Cognition • Any improvements in cognition were secondary to improvements in mood symptoms • To date, no conventional antidepressant has shown significant improvements in cognitive symptoms • MDD patients who achieve remission of other symptoms often have persistent cognitive deficits • Some antidepressants worsen cognitive deficits • Study limitations: small sample sizes; lack of replication; not always placebo-controlled; cognitive function not primary endpoint; largest studies conducted in the elderly, or in populations with large age range McIntyre RS, et al. Depress Anxiety. 2013;30:515-527; Fava M, et al. J Clin Psychiatry. 2006;67:1754-1759;Greer TL, et al. CNS Drugs. 2010;24:267-284; Herrera-Guzman I. J Affect Disord. 2010;123:341-350; McClintock SM, et al. J Clin Psychopharmacol. 2011;31:180-186; Trivedi MH, Daly EJ. Dialogues Clin Neurosci. 2008;10:377-384; Millan MJ, et al. Nat Rev Drug Discov. 2012;11:141-168.
New Multimodal Antidepressants Reuptake inhibitors + 5-HT receptor actions to add to the efficacy and/or reduce adverse effects 5-HT3 5-HT1A 5-HT1A Vilazodone Vortioxetine 5-HT1B 5-HT10 SERT SERT 5-HT7 Other multimodal drugs in development: brexpiprazole, amitifadine SERT = serotonin transporter. Nutt DJ. J Psychopharmacol. 2009;23;343-345.Richelson E. Int J Neuropharmacol. 2013;16:1433-1442.Mork A, et al. ENCP 2013. Poster P.2.e.002.
Vortioxetine Effect on Cognitive Performance Primary end point: composite z-score (DSST / RAVLTacq / RAVLTdelay) at Week 8 vs placebo (FAS, MMRM) NCT01422213 *P<.001; †P<.05; ‡P<.01; vs placebo. DSST = Digit Symbol Substitution Test; RAVLT = Rey Auditory Verbal Learning Test; acq = acquisition; delay = delayed recall; FAS = full analysis set; MMRM = mixed model for repeated measurements. *Vortioxetine is not FDA approved for treatment of cognitive impairment. McIntyre RS, et al. Int J Neuropsychopharmacol. 2014;17:1557-1567.
Preclinical Comparison of Vortioxetine, SSRIs, and SNRIs in Cognitive Function Study Assessed Cognitive Function Using Quantitative EEG Measurers and a Novel Object Recognition Memory Task in Normal and 5-HT-Depleted Rats Episodic Memory (novel object recognition test) Spatial Memory (spontaneous alteration) § § Preference Score (%) Alteration (%) PCPA PCPA Control Control Duloxetine Duloxetine Vortioxetine Vortioxetine Escitalopram Escitalopram Occupancy (%) SERT 88 >90 95 *P<.05, †P<.01, ‡P<.001 vs control; §P<.05 vs PCPA • Vortioxetine restored memory deficits induced by 5-HT depletion; escitalopram and duloxetine did not • Results suggest a role for vortioxetine in modulating cortical networks recruited during cognitive behavior EEG = electroencephalography; PCPA = 4-chloro-DL-phenylalanine Mork A, et al. ECNP 2013. Poster P.2.e.002.
Long-term Safety and Tolerability of Vortioxetine 52-Week, Long-term, Open-Label, Flexible-Dose Extension Study of Vortioxetine 15 or 20 mg/day TEAEs reported by at least 5 patients (N=71) Similar long-term adverse event profile to that observed during short-term treatment TEAEs = treatment-emergent adverse events. Filippov G, et al. ENCP 2013. Poster P.2.b.011.
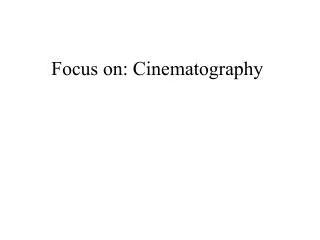
Frampton JE. CNS Drugs. 2011;25:615-627. Safety and Tolerability of Vilazodone 30 Vilazodone(n=436) 25 Placebo (n=433) 20 Incidence (% of patients) 15 10 5 0 Fatigue Nausea Anxiety Diarrhea Vomiting Dizziness Insomnia BackPain Headache DryMouth Somnolence Nasopharyngitis Weight Increased Abnormal Dreams Increased Appetite Upper Respiratory Tract Infection Short-term tolerability of oral vilazodone in adult patients with MDD.Incidence of treatment-emergent adverse events occurring in ≥5% of vilazodone patients.40-mg, once-daily recipients in two 8-week, double-blind, placebo-controlled studies (pooled results).
Investigational Compounds With Potential Procognitive Effect • Modafinil • Considered an effective augmentation strategy for both acute unipolar or bipolar depressive episodes1 • 4-week, open-label study in 35 patients with a history of MDD2 • Partial response of depressive symptoms; some improvement of cognitive function • Donepezil • Available evidence to date does not suggest a clear benefit as adjunctive therapy to antidepressants for cognitive enhancement3 • Clinical trial to assess cognitive improvement for a large sample of cognitively impaired MDD patients with combined treatment of antidepressant/donepezil is ongoing 1. Goss AJ, et al. J Clin Psychiatry. 2013;74:1101-1107. 2. DeBattista C, et al. J Clin Psychopharmacol. 2004;24:87-90.3. Reynolds CF 3rd. Arch Gen Psychiatry. 2011;68:51-60.
Investigational Compounds With Potential Procognitive Effect (cont’d) • Ketamine • May have neuroprotective effects, including in an ECT treatment context1,2 • Additional clinical trials are ongoing • S-adenosyl-methionine (SAME-E) • Superior to placebo and comparable to tricyclic antidepressants for MDD symptoms3 • Preliminary evidence shows improved recall information and a trend toward a greater enhancement in word-finding in depressed patients treated with oral, adjunctive SAM-E4 1. Hudetz JA, Pagel PS. J CardiothoracVascAnesth. 2010;24:131-142. 2. MacPherson RD, Loo CK. J ECT. 2008;24:52-56. 3. Papakostas GI, et al. J Clin Psychiatry. 2009;70(suppl 5):18-22. 4. Levkovitz Y, et al. Eur Psychiatry. 2012;27:518-521.
Investigational Compounds With Potential Procognitive Effect (cont’d) • Erythropoietin (EPO) • Single high dose may enhance memory/executive function1 • Follow-up, randomized, double-blind, placebo-controlled study: sustained improvements in verbal learning and memory after repeated EPO administrations as adjunctive treatment (8 weekly infusions of 1 ml recombinant EPO—doses of 40,000 UI) versus placebo2 in patients with TRD • Lisdexamfetamine (LDX) • Randomized, double-blind, placebo-controlled, parallel-group study for treating executive dysfunction in patients on antidepressant therapy with full or partial remission of other symptoms • In addition to improvement of any residual depressive symptomatology, patients treated with LDX displayed greater executive improvement compared with placebo 1. Miskowiak KW, et al. Psychopharmacology (Berl). 2012;219:687-698. 2. Miskowiak KW, et al. Biol Psychiatry. 2014 Dec 18. 3. Madhoo M, et al. Neuropsychopharmacology. 2014;39:1388-1398.
Alternative Therapeutic Strategies to Address Cognitive Symptoms ↑ = improvement; ↓ = worsening; ± = no marked change. Millan ML, et al. Nat Rev Drug Discov. 2012;11:141-168.
Targeting Cognitive Deficits in MDD: Cognitive Remediation • Potential aim: to exercise specific pathways with the goal of remediating specific areas of cognitive function • Methods: using behavioral strategies to improve a range of neuropsychologic domains, such as memory and executive functioning • Techniques: cognitive control training sessions, computer games, group discussion, homework, application to real-life situations Bowie CR, et al. J NervMent Dis. 2013;201:680-685.
Trivedi MH. J Clin Psychiatry. 2009;70(suppl 6):26-31. American Psychiatric Association. http://psychiatryonline.org/data/Books/prac/PG_Depression3rdEd.pdf. Accessed March 30, 2015. Measurement-Based Care for MDD • Systematically use measurement tools to monitor progress and guide treatment choices • Regularly scheduled visits • Time-efficient, validated tools • Regularly monitoring symptom improvement, side effects, medication adherence • Use a treatment algorithm with established critical decision points
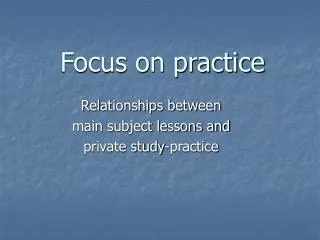
HRSD = Hamilton Rating Scale for Depression. Geerts E, et al. J Affect Disord. 1996;40:15-21. Krupnick JL, et al. J Consult Clin Psychol. 1996;64:532-539. Establishing a Therapeutic Alliance Early inTreatment Is a Powerful Remission Tool 35 Β=.46, P=.009 30 25 20 Improvement (HRSD T1–T2) 15 10 5 0 -5 -0.5 1.0 -1.0 0.0 0.5 -1.5 Change of Attunement During First Clinical Interview
Summary • Cognitive symptoms of MDD are especially difficult to treat and frequently persist even when patients are otherwise responsive to an antidepressant • Traditional antidepressants frequently failed to adequately address cognition • New multimodal antidepressants appear to be particularly efficacious in targeting the residual symptoms of MDD, particularly in regard to cognitive deficits, with favorable side-effect profiles • However, not all patients may be candidates for these therapies; individualization of therapy is key
Summary (cont’d) • Alternative approaches—especially cognitive therapy—may be helpful • The goal of MDD remains: remission of all symptoms, including cognition • It is critical to continuously monitor therapeutic response and make adjustments accordingly • A number of validated instruments have been developed to facilitate monitoring of response • As with any chronic disease, the patient-provider relationship is paramount for good outcomes