Numerical Chromosome Abnormalities
Numerical Chromosome Abnormalities. Group 5: Dean Sevel , Gail Feller, Maheshen Padayachee , Tamaryn Fox, Bracha Katz, Elan Milwid, Michell Gow , Keevan Naicker , Faheem Meer, Bianca Koeller. INTRODUCTION. Normal female: 46,XX Normal male 46,XY. Numerical Chromosome Abnormalities:

Numerical Chromosome Abnormalities
E N D
Presentation Transcript
Numerical Chromosome Abnormalities Group 5: Dean Sevel, Gail Feller, MaheshenPadayachee, Tamaryn Fox, Bracha Katz, Elan Milwid, MichellGow, KeevanNaicker, Faheem Meer, Bianca Koeller
INTRODUCTION Normal female: 46,XX Normal male 46,XY Numerical Chromosome Abnormalities: “Any karyotype where the number of chromosomes present in a single cell differs from the norm of 46 in humans”.
Chromosome Abnormalities • A chromosome abnormality may reflect either: • an incorrect number of chromosomes • a structural abnormality in one or more chromosomes • Numerical Chromosome Abnormalities • Most irregular chromosome numbers are the result of non-disjunction - a failure of meiosis in the production of sperm and ova • About 20% of all human conceptions carry a chromosomal defect • Generally, 6/1000 new-born babies carry a chromosomal abnormality
Presentation of Chromosomal Abnormalities Spontaneous Abortions Defects in Newborns
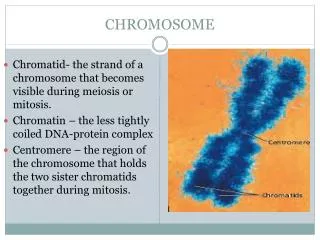
Types of Numerical Chromosome Abnormalities Aneuploidy: occurrence of one or more extra or missing chromosomes leading to an unbalanced chromosome complement. Occurs by nondisjunction Loss of a single chromosome: (2n-1) = monosomy Gain of a single chromosome (2n+1) = trisomy
Monosomy Monosomy is a form of aneuploidy. Characterised by the presence of only one chromosome from the homologous pairs. Partial monosomy occurs when only a portion of a chromosome is missing from the genome of an individual. All autosomal monosomies are lethal and affected foetuses will not survive development.
Turner syndrome • Turner syndrome is the only full monosomy that is seen in living individuals • It is characterised by one X chromosome (Genotype: XO) • Karyotype = 45, XO • Only affects females • Some symptoms include a short statue, swollen hands and feet, and a collection of unique facial features • Note: Turner syndrome is an example of an X linked monosomy and not an autosomal monosomy.
Partial Monosomy • Most partial monosomies are caused by deletions on chromosomes. • Examples: Cri-du-chat syndrome, DiGeorge syndrome, Prader-Willi syndrome
Cric-du-chat syndrome • Caused by deletion on p arm of chromosome 5 • Symptoms include: difficulty swallowing, a distinctive cry, poor growth, and severe cognitive, speech and motor delays.
Statistics • Turner syndrome: 1 in 2500 births. Average height of affected females is 4 ft 8 in • Cri-du-chat syndrome: Common deletion seen. 1 in 35 000 births. Deletion occurs during crossing over of meiosis.
Types of Numerical Chromosome Abnormalities • Polyploidy • Process of the genome doubling • “ploidy” refers to the number of complete genomes contained in a single cell. • Polyploidy can arise form nondisjunction of homologous chromosomes during meiosis resulting in diploid gametes. • “digyny” vs. “diandry” • Triploidy = 69 chromosomes • Tetraploidy = 92 chromosomes • Vast majority of triploid conceptions end as miscarriages, those that survive usually die shortly after birth.
Nondisjunction • The failure of chromosome pairs to separate properly during meiosis or mitosis. • Could arise from: • a failure of homologous chromosomes to separate in meiosis I • Failure of sister chromatids to separate during meiosis II or mitosis • Increase in maternal age is result is an increased frequency of this occurring.
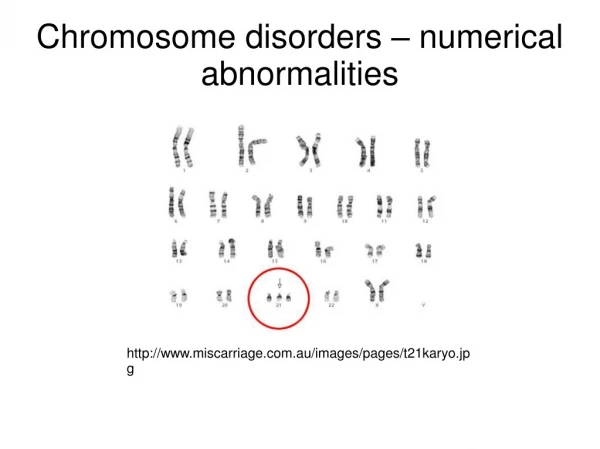
Down Syndrome • Background • Also referred to as trisomy 21 • The disease is a chromosomal abnormality caused by the addition of all or part of an extra 21st chromosome. • Named after John Down, the physician who identified the disease in 1866 • 3 different types of Down Syndrome namely: a trisomy 21 caused by non-disjunction, a mosaic type and a Robertsonian translocation type • Epidemiology • The incidence is one in 800 to 1000 births • 95% of the cases are trisomy 21 cases, 1-2% are mosaic cases and 2-3% are Robertsonian Translocation cases • The maternal age has an impact on the risk of having a child with Down Syndrome. Between 20 to 24, the probability is one in 1562, between ages 35 to 39 the probability is one in 214, and above the age of 45 the probability is one in 19. • In recent data it is suggested that paternal age over 42 is also likely to be a cause of Down Syndrome
Down Syndrome • Symptoms and Characteristics • Short Stature and hypotonia • Single Palmer Crease called a Simian line • Small/low ears, tongue projects out of mouth due to narrow palate and epicanthal folds • Impaired Intellectual and Cognitive Ability • Possible heart disease and hypothyroidism • Small head, upward slanting eyes and flattened facial features • Wide gap between big toe and rest of toes • Treatment • No cures but there are treatments to control symptoms • Control of hypertension and repair of congenital heart defects • Counselling and support • Possible plastic surgery if it is vital
Down Syndrome The genetics behind…. • Trisomy 21 • Trisomy 21 (47,XX,+21) • Caused by non-disjunction event, a gamete (sperm or egg) is produced with an extra chromosome 21 (has 24 chromosomes) and thus the zygote it produces has 47 chromosomes • Accounts for 95% of Down Syndrome cases, 88% occurs in maternal egg non-disjunction while 8% occurs in paternal sperm non-disjunction • Mosaicism • (46,XX/47,XX,+21). • Some of the cells in the body are normal and some are trisomy 21 = 2 cell lines • Can occur either by: • a non-disjunction during an early mitosis in a normal embryo which results in some of the cells having trisomy 21 • a Down syndrome embryo undergoes non-disjunction and some of the cells revert to the normal chromosomal array. • The ratio of normal cells to trisomy 21 cells is variable • 1-2% of Downs Cases • Studies show slight improvement in mosaic DS from normal DS
Down Syndrome The genetics behind…. • Robersonian Translocation • [45,XX,der(14;21)(q10;q10)] (1421 translocation) • In parent the long arm (q arm) of chromosome 21 is attached to long arm of another chromosome (often chromosome 14) = phenotypically normal. • Non-disjunction (unbalanced) during replication leads to increased chance of creating a gamete with an extra 21 chromosome = down syndrome in progeny • Maternal/Paternal age does not have an effect on this type • Screening and Prevention • Mother and Father can be genetically screened to determine risk • Amniocentesis (amniotic fluid test), Chorionic Villus Sampling, Percutaneous Umbilical Cord Blood sampling • Counselling for parents • Option of pregnancy termination (ethical issues)
Down Syndrome Down Syndrome as a result of maternal Robertsonian translocation
Trisomy 13- Patau’s Syndrome Background Occurs as a consequence of non- disjunction of chromosome 13 during meiosis Incidence and Recurrence 2 per 10000 live births Symptoms Microcephaly (abnormally small head and underdeveloped brain) Polydactyly Low-set ears Cleft palate lip Structural eye abnormalities/ defects Kidney and heart defects (especially of the ventricular septum) Treatment: Patau’s Syndrome is managed on a case-by- case basis which is dependent on the severity of the symptoms presented by the affected individual. Corrective surgery can be used to rectify problems such as the cleft palate and the septal defects of the heart.
Numerical Sex Chromosome Abnormalities • General • Sex Chromosome aneuploidies • Their symptoms are typically less severe than those of diseases caused by autosomal aneuploidies • Tend to occur less frequently than their autosomal counterparts Female Sex Chromosome Abnormalities Turner Syndrome (XO) • Monosomy of the X chromosome in a female • Affected females typically have a short stature, a webbed neck, underdeveloped gonadal structures and low- set ears Triple X syndrome (also known as Trisomy X) • Female inherits 3 X chromosomes. In rarer instances the female can inherit more than 1 additional X chromosome. • Females with trisomy X usually do not present any significant symptoms because 2 of the 3 X chromosomes are inactivated by non-coding RNA (XIST gene). However in rare instances females with trisomy X can suffer from behavioral problems, poor cordination, mental retardation and infertility
Male Sex Chromosome Abnormalities Klinefelter’s Syndrome • Not an Aneuploidy of the Y chromosome rather males Inherit one or more X chromosomes • (47,XXY) is the most common Klinefelter genotype • Affected individuals are phenotypically male but they do exhibit some female secondary sexual characteristics at puberty • Other symptoms include: hypogonadism (insufficient Testosterone production), infertility, gynecomastia (increased breast development) and learning disabilities • Treatment includes testosterone treatment for individuals who desire a more masculine appearance • Incidence: 1 in 1000 male births XYY Syndrome • Aneuploidy of the Y chromosome in which males inherit an additional Y chromosome • Common Symptoms: Increased growth rate during childhood, predisposition to learning disabilities and impaired language skills • Incidence: 1 in 1000 to 1 in 2000 male births
Edward’s Syndrome (trisomy 18) • 2nd most common trisomy after Down syndrome that is carried to term. • Occurs by nondisjunction • characteristics: • Kidney malformations • Structural heart defects • Severe mental retardation • Intestines protruding outside body • Developmental delays • Growth deficiency
Physical Malformations of Edward’s Syndrome Digits 2 and 5 overlap 3 and 4
Links Between Advanced Maternal Age and Numerical Chromosome Abnormalities • All the eggs a woman will possess in her lifetime were present since before she was born. • As a woman ages, the DNA contained within the eggs becomes less stable. • When women are in the peri-menopausal state of their lives, the eggs are less responsive due to the highly variable hormonal fluctuations. • Thus advanced maternal age leads to a higher risk of chromosomal abnormalities.
Integration • Embryology and Numerical Chromosome disorders • Trisomy 21 can cause an atrioventricularseptal defect (endocardial cushion defect) • Malfunction of lip and palate formation occurs in Patau’s syndrome which presents as a cleft lip and/or palate.
Physiology and Numerical Chromosome Disorders Increased risk for dysfunction of the thyroid gland
Images/Info Courtesy of: • http://www.medicinenet.com/down_syndrome/article.htm • http://writergrasshopper.wordpress.com/2011/03/13/karyotipe-and-down-syndrome/ • http://www.pmlf.org/cancer/down-syndrome-would-provide-new-options-for-cancer-treatment-335.html/attachment/down-syndrome • http://www.downsyndrome.org.za/ • Google Images