Download

1 / 93
1.5k likes | 4.85k Vues
Respiratory Diseases of the Newborn. Beth Mogensen, RRT-NPS. OBJECTIVES. Provide overview of respiratory system of the newborn Identify non-respiratory causes of distress in the newborn Review respiratory diseases/ anomalies of the newborn. Early Development. Fetal Lung Development.

E N D
Respiratory Diseases of the Newborn Beth Mogensen, RRT-NPS
OBJECTIVES • Provide overview of respiratory system of the newborn • Identify non-respiratory causes of distress in the newborn • Review respiratory diseases/ anomalies of the newborn
Fetal Lung Development • Week 4: the laryngotracheal groove forms on the floor foregut • Week 5: the left and right lung buds push into the pericardioperitoneal canals (primordial of pleural cavity) • Week 6: the descent of heart and lungs into the thorax. Pleuroperitoneal foramen closes
Week 7: the lung buds divide into secondary and tertiary bronchi Week 24: the bronchi divide 14 more times and the respiratory bronchioles develop By birth, there will be an additional 7 divisions of bronchi Fetal Lung Development
STAGE 1: Pseudoglandular Period (5-17 weeks) all the major elements of the lungs have formed except for those involved with gas exchange STAGE 2: Canalicular Period (16-25 weeks) bronchi and terminal bronchioles increase in lumen size and the lungs become vascularized Fetal Lung Histology
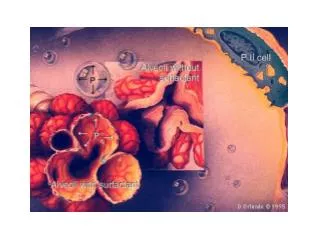
Fetal Lung Histology • STAGE 3: Terminal Sac Period (24 weeks to birth) more terminal sacs develop and interface with capillaries lined with Type I alveolar cells or pneumocytes --Also have Type II pneumocytes which secrete surfactant thereby decreasing the surface tension forces and aids in expansion of the terminal sacs
STAGE 4: Alveolar Period (late fetal period to 8 years) 95% of mature alveoli develop after birth. A newborn has only 1/6 to 1/8 of the adult number of alveoli and lungs appear denser on x-ray
Respiratory Distress at Birth Rule of 6: non respiratory causes of distress S & S Diagnosis Management • Hypothermia/ - check temperature - heat or cool as Hyperthermia necessary • Hypovolemia - obtain prenatal history - gingerly give volume • Hyoptension - measure blood pressure - give volume and/or vasopressor • Hypoglycemia - blood glucose measurement - give glucose • Anemia - measure hematocrit - transfuse with PRBC • Polycythemia - measure hematocrit - partial exchange transfusion (lower Hct)
Respiratory Distress in the Newborn • Transient Tachypnea of the Newborn (TTN) • Surfactant Deficiency (HMD,RDS) • Meconium Aspiration Syndrome (MAS) • Pneumonia/ Sepsis • Pneumothorax or other air leaks
Respiratory Distress in the Newborn Respiratory Causes • Congenital Abnormalities of the Lung/Thorax • Congenital Heart Disease (CHD) • Congenital Diaphragmatic Hernia (CDH) • Congenital Cystic Adenomatiod Malformation (CCAM) • Tracheal Abnormalities • Esophageal Atresia • Pulmonary Hypoplasia • Persistent Pulmonary Hypertension of the Newborn (PPHN)
What do you need to knowto Figure out the Cause… • Maternal History • Any risk factors • Gestational age of Infant • Amniotic fluid (color/odor/volume) • Intrapartum history • Clinical Presentation/ Assessment • X-Rays • Lab Evaluations
Clinical Presentation • Respiratory Assessment • Respiratory rate • Quality • Shallow • Deep • Nasal Flaring • Grunting • Retractions • Breath Sounds
Clinical Presentation • Color—pink, dusky, pale, mottled • Central • Peripherally • Heart rate • Pulses • Distal vs Central • Perfusion • Capillary Refill Time (CRT) • Blood Pressure
Clinical Presentation • Physical characteristics • Flat nasal bridge, Simian crease, recessed chin, low set ears • Deformities • Extra digits, gastroschesis, imperforate anus • Muscular • Hyoptonia vs Hypertonia • Skeleton • Choanal Atresia, Osteogenesis Imperfecta • Other • Scaphoid abdomen, heart tones on Right side
X-Ray • Structures • Ribs • Vertebra • Liver • Stomach/ intestine • Lungs • Heart • Trachea • Esophagus
X-Ray • Lungs • Lung Volume • Expansion • Densities • Fluid/ collapse (atelectasis)>>white • Free Air>>dark • Mass • Heart shape and size • Boot shaped • Egg or Oval shaped
Lab Values • CBC with diff • ABG/CBG/VBG • Blood Cultures • CRP • Electrolytes • Type and Cross • PKU
Respiratory Distress Determining Differential Diagnosis What you need to know… • History • Presentation/ clinical assessment • X-rays • Lab values
Transient Tachypnea of the Newborn (TTN) • Most common diagnosis of respiratory distress in the newborn • Remember often “term infants” may be a little early • Ineffective clearance of amniotic fluid from lungs with delivery • Most often seen at birth or shortly after
Transient Tachypnea of the Newborn • History • Common with C-Section delivery • Maternal analgesia • Maternal anesthesia during labor • Maternal fluid administration • Maternal asthma, diabetes, bleeding • Perinatal asphyxia • Prolapsed cord
TTN presents: • Respiratory Assessment • Tachypnea 60-150 bpm • Nasal flaring • Grunting • Retracting • Fine Rales • Cyanotic
TTN • X-Ray findings • Prominent Perihilar streaking • Hyperinflation • Fluid in fissure • Labs • CBC within normal limits • ABG/CBG showing mild to moderate hypercapnia, hypoxemia with a respiratory acidosis
TTN • Have delayed reabsorption of fetal lung fluid which eventually will clear over several hours to days • Treatment: Treat signs and symptoms. Support infant, may need O2, is probably too tachypneic to PO feed so start IV fluids • Be patient!!
Surfactant Deficiency (RDS, HMD) • One of the most common problems associated with a premature infant • Decreased surfactant production in lungs of pre-term infants • With decreased surfactant production, alveoli collapse, become atelectatic, yielding poor lung function and increasing signs of respiratory distress
RDS • History • Gestational age < 38 weeks • Prenatal care • Diabetes (controlled vs uncontrolled) • Perinatal infection • Problems during pregnancy/delivery • Asphyxia • Stress to fetus • Hypothyroidism • Multiple births
RDS presents: • Respiratory Assessment • Tachypnea > 60 bpm • Nasal flaring • Grunting • Retracting • Apnea/ irregular respiratory pattern • Rales (crackles) • Diminished breath sounds • Cyanosis
RDS • X-Ray • Loss of volume • Reticulogranular pattern or “ground glass” appearance • Air bronchograms • Bell shaped thorax • Air leak, PIE • Loss of heart borders/ atelectasis • White out
RDS • Laboratory Results • ABG/CBG • Hypoxia • Hypercarbia • Acidosis • CBC with Differential/ HHP • Used to rule out other causes of respiratory distress • Always check electrolytes, especially glucose, potassium and calcium
Treatment for RDS • Post-Exogenous Surfactant Therapy • Many on the market • Prophylactic Treatment • Administered in the delivery room • Rescue Treatment • Given after a definitive diagnosis of RDS
MECONIUM ASPIRATION SYNDROME • Most often found in post date infants > 40 weeks, but may occur in infants >34 weeks • Infant passes meconium due to varying degrees of asphyxia in utero • Obstruction of large and small airways with aspirated meconium • Aspiration may occur: • in utero • intrapartum • postpartum period
MAS • History • Prenatal Care • Maternal diabetes • Pregnancy Induced Hypertension (PIH) • Pre-eclampsia • Problems during pregnancy/delivery • Color of amniotic fluid
MAS • Respiratory Assessment • Tachypnea • Nasal flaring • Grunting • Retracting • Apnea/ irregular respiratory pattern • Decreased breath sounds/ wet/ rhonchi
MAS • Clinical Assessment • Color • Pale/gray • Cyanotic • Stained skin • X-Ray • Increased AP diameter • Hyperinflation • Atelectasis • Pneumothorax
Pneumonia/ Sepsis • Occurs frequently in newborns • 3 types • Congenital Pneumonia • Intrapartum Pneumonia • Postnatal Pneumonia • Most often seen with chorioamnionitis, prematurity and meconium aspiration • Get thorough history
Causes • Prematurity • Prolonged rupture of membranes • Maternal temp > 38C • Foul smelling amniotic fluid • Nonreassuring stress test • Fetal tachycardia • Meconium • Maternal hx of STDs
Respiratory Assessment • Tachypnea • Apnea, irregular breathing pattern • Grunting • Retractions • Nasal flaring • Colorful secretions • Rales, rhonchi • Cyanosis
Clinical Assessment • Gray, pale color • Lethargy • Temperature instability • Skin rash-pettechia • Tachycardia • Glucose issues • Hypoperfusion • Oliguria
X-Ray • Patchy infiltrates (aspiration) • Bilateral diffuse granular pattern • Streaky • Loss of volume • Densities
Pneumothorax and otherAir Leaks • History • What happened in the delivery room? • Was positive pressure given? • Large amount of negative pressure generated with the 1st breath?
Pneumothorax/ Air Leaks • Respiratory Assessment • Tachypnea • Nasal flaring • Grunting • Retractions • BS absent or decreased