Disorders of the Pituitary and Hypothalamus
Disorders of the Pituitary and Hypothalamus. Hasan AYDIN, MD Yeditepe University Medical faculty Department of Endocrinology and Metabolism. Pituitary Hormones. Endocrine Diseases. Pituitary Diseases. Diabetes Insipidus Inappropriate ADH Syndrome Empty Sella Syndrome

Disorders of the Pituitary and Hypothalamus
E N D
Presentation Transcript
Disorders of the Pituitary and Hypothalamus Hasan AYDIN, MD Yeditepe University Medical faculty Department of Endocrinology and Metabolism
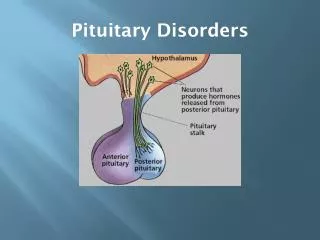
Pituitary Diseases • Diabetes Insipidus • Inappropriate ADH Syndrome • Empty Sella Syndrome • Hyperpituitarism • Hypopituitarism • Pituitary Apoplexy • Pituitary Neoplasms
Pituitary Adenomas • Account for 10 % of all intracranial tumors • Almost always benign • Frequently seen after the third decade • Should be differentiated from • Hyperplasia • Craniopharyngiomas (from Rathke’s pouch) • Meningiomas,malignant tumors, cysts,abscess • Lymphocytic hypophysitis • Microadenoma < 1 cm • Macroadenoma > 1 cm
Pituitary Tumors: Clinical Presentation • Mass effect • Superior extension • May compromise optic pathways – leading to impaired visual acuity and visual field defects • May produce hypothalamic syndrome – disturbed thirst, satiety, sleep, and temperature regulation • Lateral extension • May compress cranial nerves III, IV, V, and VI – leaning to diplopia • Inferior extension • May lead to cerebrospinal fluid rhinorrhea • Hormone defiency • Hypopituitarism • Diabetes insipitus • Hormone excess • Hyperpituitarism • Inappropriate secretion of ADH
Etiology of Pituitary Adenomas • Non-Functioning Pituitary Adenomas • Endocrine active pituitary adenomas • Prolactinoma • Somatotropinoma • Corticotropinoma • Thyrotropinoma • Other mixed endocrine active adenomas • Malignant pituitary tumors: Functional and non-functional pituitary carcinoma • Metastases in the pituitary (breast, lung, stomach, kidney) • Pituitary cysts: Rathke's cleft cyst, Mucocoeles, Others • Empty sella syndrome
Etiology of Pituitary Adenomas • Developmental abnormalities: Craniopharyngioma (occasionally intrasellar location), Germinoma, Others • Primary Tumors of the central nervous system: Perisellar meningioma, Optic glioma • Vascular tumors: Hemangioblastoma • Malignant systemic diseases: Hodgkin's disease, Non-Hodgkin lymphoma, Leukemic infiltration, Histiocystosis X, Eosinophilic granuloma, Giant cell granuloma (tumor) • Granulomatous diseases: Neurosarcoidosis, Wegener's granulomatosis, Tuberculosis, Syphilis • Vascular aneurysms (intrasellar location)
Evaluation of an Incidental Pituitary Mass • Clinical Evaluation • Hormonal Evaluation • Radiologic Evaluation
Clinical Evaluation • Inappropriate pituitary hormone secretion • Visual field deficits • Cranial nerve palsies • Temporal lobe epilepsy • Hydrocephalus • Cerebrospinal fluid rhinorrhea
Hormonal Evaluation • Mayinclude of both basal hormone measurement and dynamic stimulation testing. • All pituitary masses should have screening basal hormone measurements, including: • Prolactin • TSH, FT4 • ACTH, AM cortisol, midnight salivary cortisol • LH, FSH, estradiol or testosterone • GH, Insulin-like growth factor-1 (IGF-1)
Hormonal Evaluation(continued) Dynamic stimulation/suppression testing: • may be useful in selected cases to further evaluate pituitary reserve and/or for pituitary hyperfunction • Dexamethasone suppression testing • Oral glucose GH suppression test • GHRH, L-dopa, arginine test • CRH stimulation test • Metyrapone test • TRH stimulation test • GnRH stimulation test • Insulin-induced hypoglycemia test
Radiologic Evaluation: MRI • Preferred imaging study for the pituitary • Better visualization of soft tissues and vascular structures than CT • No exposure to ionizing radiation
Radiologic Evaluation: CT • Better at visualizing bony structures and calcifications within soft tissues • Better at determining diagnosis of tumors with calcification, such as germinomas, craniopharyngiomas, and meningiomas • May be useful when MRI is contraindicated, such as in patients with pacemakers or metallic implants in the brain or eyes • Disadvantages include: • less optimal soft tissue imaging compared to MRI • exposure to radiation
Management of Pituitary Neoplasia • Observation • Pharmacotherapy • Surgery • Radiation Therapy
Pituitary Incidentaloma < 10 mm > 10 mm • Evaluate for: • Hormonal Hypersecretion • Hormonal Hyposecretion • Visual Changes/defects Evaluate for Hormonal Hypersecretion Hormonal or Visual Abnormalities Normal No Abnormalities Observe Treatment Observe
Observation and Follow-up • If less than 20 mm and no neurologic or hormonal abnormalities: • Monitor for adenoma size, visual changes, and hormonal hypersecretion in 6 and 12 months, then annually for a few years • Lesions less than 10 mm and proven to have no hormonal hypersecretion: • Lesions 2 to 4 mm: no further testing required • Lesions 5 to 9 mm: MRI can be done once or twice over the subsequent two years; if the lesion is stable in this period, the frequency can be decreased
Pharmacotherapy Which pharmacologic option to choose depends on type of tumor: • Dopamine agonists:Bromocriptine, Cabergoline- most useful for prolactinomas, less useful for GH secreting adenomas • Somatostatin analog: (Octreotide, Octreotide LAR, Lanreotide)- most useful for acromegaly • Pegvisomant (GH receptor blocker): useful in acromegaly refractory to somatostatin analogues • Other:Ketoconazole, Metyrapone, Mitotane- for Cushings disease- use limited by side effects, expense and lack of efficacy
Pituitary Surgery • Transsphenoidal approach: used for 95% of pituitary tumors • Endonasal submucosal transseptal approach • Septal Pushover/Direct Sphenoidotomy • Endoscopic approach
Indications for Surgery • First-line treatment of some symptomatic pituitary adenomas. • Useful when medical therapy fails • Indicated in pituitary apoplexy with compressive symptoms • Surgery provides prompt relief from excess hormone secretion and mass effect.
Radiation Therapy • Reserved for patients with larger tumors and/or persistent hormonal hyperfunction despite surgical intervention • Conventional radiotherapy • Gamma knife radiosurgery
Conventional Radiotherapy • Response is slow, may take 5 to 10 years for full effect • Successful in up to 80% of acromegalics and 55-60% of Cushing’s disease • High rate of hypopituitarism: up to 60% • Other complications: optic nerve damage, seizures, radionecrosis of brain tissue
Gamma/Cyber Knife Radiosurgery • Stereotactic CT guided cobalt 60 gamma radiation to narrowly focused area • Long term data not yet available but suggest up to a 70% response rate for acromegaly and up to 70% for Cushing’s in some centers • Complication rate likely lower, but still high rate of hypopituitarism (~55%)
Abnormal Pituitary Function Associated with Pituitary Tumors
Disorders of Pituitary Function • Hypopituitarism • Central hypoadrenalism, hypogonadism, hypothyroidism or GH deficiency • Panhypopituitarism • Hypersecretion of Pituitary Hormones • Hyperprolactinemia • Acromegaly • Cushing’s Disease
Prolactinoma • Most common functional pituitary tumor • 25-30% of all pituitary adenomas • Some growth hormone (GH)–producing tumors also co-secrete PRL • Usually a microadenoma • Of women with prolactinomas- 90% present with microprolactinomas • Of men with prolactinomas- up to 60% present with macroprolactinomas • Although many women with hyperprolactinemia will have galactorrhea and/ or amenorrhea • The absence these the two signs do not exclude the diagnosis • GnRH release is decreased in direct response to elevated prolactin, leading to decreased production of LH and FSH
Signs and symptoms of prolactinomas • Galactorrhea • Oligomenorrhea or amenorrhea • Reduced fertility • Loss of libido • Erectile dysfunction • Headache • Visual field deficits
REMEMBER Not all hyperprolactinemia is due to a prolactinoma
Diagnostic Investigation • Measurement of random PRL levels at any time of day • History/physical examination • Pregnancy test, thyroid ve renal function tests • MRI (CT) • Visual field examination • Anterior hypophyseal function tests
Misleading Prolactin Measurements • “Hook effect” • Macroprolactinemia
“Hook Effect” If there is a very high circulating concentration of prolactin, the excess number of prolactin molecules may consume or saturate added first antibody so that there none of the molecules of prolactin can attach to the fixed or second antibody.
Macroprolactinemia • Prolactin forms • Prehormone (25,000 kDa) → Monomeric form (23000kDa) • Big PRL (50,000 kDa) • Big big PRL (MW > 100,000 kDa): monomeric PRL + IgG antigen-antibody complex • Incidence • 10 % in endocrinology practice • 18-42 % in the serum of patients with hyperprolactinmia • Patients with macroprolactinemia • Most have no typical symptoms • ⅓ of patients with amenorrhea, galactorea, infertility • Does not exclude presence of pituitary adenoma • Supressive effect of bromocriptine is partial and late
Macroprolactinemia Diagnosis • Gel filtration chromatography • Time taking, expensive and not universal • Polyethylene glycol (PEG) precipitation • Macroprolactine precipitates • In the supernatant • 60 % recovery → monomeric PRL • 40 % and less recovery → macroprolactinemia • 40 – 60 % → monomeric, oligomeric, macro
Prolactinoma Treatment • Factors effecting treatment decision • Tumor size • Gonadal dysfunction • Fertility • Gold standart is dopamin agonists • Bromocriptine (ergot derivatives) • Cabergoline (nonergot agonist) • Transsphenoidal surgery • Cure rate low, recurrence frequent
Comparison of carbergoline, pergolide and bromocriptine therapies
Dopamine Agonists • Bromocriptine- start low dose at 1.25- 2.5 mg day at night before increasing to 2.5 – 10 mg per day in divided doses. Take with food to reduce side effects. • Cabergoline- more effective and with less side effects than Bromocriptine but also more expensive- given once or twice a week with a starting dose of 0.25 mg 2 x week Titrate these based on prolactin levels and tolerability
Acromegaly • Caused by GH excess from the pituitary • Incidence 3-4/million/year • MEN-1, McCune Albright Syndrome, Familial, Carney Complex • Diagnosis 6-10 years after the onset of disease
Lesions associated with excessive secretion of growth hormone (GH) • Hypothalamic • GRF producing tumors • Gangliocytoma(hamartoma,choristoma) • with pituitary adenoma • with GH cell hyperplasia • Hypophyseal (anterior pituitary) • GH producing adenoma • GH cell hyperplasia and associated with hypothalamic,hypophyseal • or ectopic GRF-producing tumor) • Intrasellar GRF-producing gangliocytoma • Ectopic • GRF-producing tumors • GH producing tumors
Manifestations of Acromegaly • GH excess • Disturbances of other hormones • Parasellar manifestations
Acral growth Prognathism Weight gain Hypermetabolism Hyperhidrosis IGT / DM Arthritic complaints Osteoporosis Soft tissue growth Hypertrichosis Pigmentation Fibroma mollescum Visceromegaly Goiter GH Excess
Dısturbances of Other Hormones • Galactorrhea • Hyperadrenocorticism • Hyperthyroidism • Increased libido • Decreased libido, male
Parasellar Manifestations • Enlarged sella • Headache • Visual impairment • Uncinate fits • Rhinorrhea • Pituitary apoplexy • Papilledema