Download
1 / 40
410 likes | 648 Vues
Explore inborn errors of phenylalanine and tyrosine metabolism, including causes, consequences, diagnosis, and treatment options like low-phenylalanine diet, BH4 supplementation, and genetic screening.

E N D
Disorders of aromatic amino acid metabolism(Phenylalanine, tyrosine) Dr. Ketki KAssistant Professor Department of Biochemistry
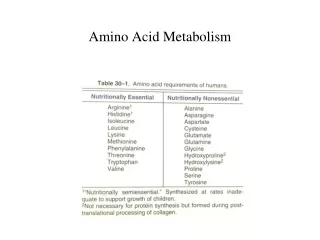
IEM • Cause: Mutant genes results in • Abnormal enzyme/ • Total loss of enzyme activity/ • Partial deficiency of enzyme • Further leads to accumulation of substrate & • No product formation
IEM of Phe & Tyr • Phenylketonuria (PKU) • Alkaptonuria • Tyrosinemia • Albinism
PKU • Most common IEM, Autosomal Recessive • Incidence- 1: 10,000 • Types: • Type I- Classical: deficiency of Phenylalanine hydroxylase • Type II & III: deficiency of Dihydro biopterin reducase • Type IV & V : deficiency of enzyme synthesizing biopterin
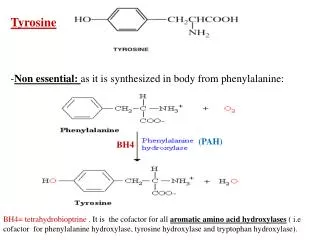
BH4 required for • Phenylalanine hydroxylase = synthesis of tyrosine • tyrosine hydroxylase = synthesis of catecholamines(NT) • tryptophan hydroxylase = synthesis of Serotonin • Deficiency of BH4 leads to ↓ tyrosine, dopamine,serotonin in brain
1) Hyperphenylalaninemia (>20 mg/dL) ↑ phenylalnine in tissue, plasma,urine 2)↑phenyllactate,phenylacetate,phenylpyruvate excreted in urine • These metabolites give urine : "mousy" odor.
C/F • Mental Retardation (low IQ<50),intellectual disability (low IQ),developmental delay, microcephaly, hyperactivity,seizures,agitation • Hypopigmentation (elevated phenylalanine competitively inhibits tyrosinase & impairs melanin formation) that causes light skin color,fair hair, blue eyes etc • Mousy body odor (due to presence of phenyllactic acid in sweat)
Laboratory diagnosis & screening • Blood phenylalanine: Normal level 1 mg/dL In PKU, level > 20 mg/dL diagnosed by chromatography, Tandem mass spectroscopy (TMS) Time of blood collection in new born: 24-48 hrs after protein feeding/breast feeding (to avoid false negative results)
2) Ferric chloride test: blue-green 3) Guthrie’s test: blood/urine: b. subtilis 4) DNPH test : Yellow ppt 5) HPLC 6) Prenatal diagnosis by using : cultured amniotic cells
Treatment 1) Diet low in phenylalanine (tapioca/cassava)/ synthetic amino acid preparation free of phenylalanine supplemented with some natural foods (fruits,vegetables, cereals) selected for their low phenylalanine content • Treatment must begin during first 7-10 days of life to prevent neurological impairment) • Lifelong restriction of phenylalanine is recommended
2) supply tyrosine In diet 3) supplementation with BH4 & L-3,4-dihydroxyphenylalnine(L-DOPA) & 5- hydroxytryptophan Improves clinical outcome in type II,III.IV, v PKU
Maternal PKU: • Lady having PKU,but not on low Phe diet becomes pregnant • Then the offspring develops “Maternal PKU syndrome”. • It causes microcephaly & congenital heart abnormalities in fetus. • It can be prevented by dietary restriction of diet containing phenylalanine in mother prior to pregnancy & maintain throughout pregnancy
Alkaptonuria • Autosomal recessive, incidence 1 in 2,50,000 births • Metabolic defect: Deficiency of Homogentisic acid oxidase • Consequences: increased homogentisic acid in urine
C/F: • Patient asymptomatic until age 40 years • Urine gets darken on exposure to air • Dark staining of diapers indicate disease in infants • Large joint arthritis, Ochronosis (deposition of black pigment/alkapton bodies on cartilage & collagenous tissue)
Investigations: • Urine: black on standing • Ferric chloride test: green color • Benedict’s test: orange-red color • HPLC
Treatment: • Not life threatening condition so no specific treatment required • Diet low in phenylalanine & tyrosine
Albinism • Autosomal recessive, Incidence: 1 in 20,000 • Due to deficiency in synthesis of pigment melanin which is due to absence of tyrosinase (copper containing enzyme) in eye & skin [ c/a tyrosinase negative oculocutaneous albinism ]
Hypopigmentation of skin, fundus & iris • Associated Photophobia,nystagmus,↓ visual acuity • Skin sensitivity to sunlight, prone to skin cancer(melanoma)
Tyrosinemia 1)Type I Tyrosinemia: Hepatorenal -Tyrosenemia 2) Type II Tyrosinemia: Oculocutaneous- Tyrosenemia 3) Type III Tyrosinemia : Neonatal Tyrosenemia 4) Hawkinsinuria
1)Type I Tyrosinemia: Hepatorenal -Tyrosinemia • Also c/a tyrosinosis • AR • Incidence: 1.5 per 1,000 births • Cause: def of Fumaryl acetoacetate hydrolase
C/F: Cabbage like odor Hypoglycemia Liver failure, renal tubular dysfunction Vitamin D resistant rickets Mild Mental Retardation, Death may occur in first 6 months of life
Investigation: • Urine contains tyrosine, pHPPA,hydroxyphenyllactic acid • Serum: shows tyrosine • Treatment: • Tyrosine & phenylalanine restricted diet
Type II Tyrosinemia: Oculocutaneous- Tyrosinemia • C/a Richner-Hanhart syndrome • Cause: deficiency of tyrosine transaminase • Consequences : urinary excretion of tyrosine,tyramine • C/F: Mental retardation, dermatitis, palmoplantar keratosis, photophobia • Treatment: diet low in phe,tyr
Type III Tyrosinemia : Neonatal Tyrosinemia Due to def of p-hydroxy phenylpyruvate hydroxylase Temporary condition Overcome by treatment with ascorbic acid
Hawkinsinuria • Autosomal dominant • Due to def of p-HPPA oxidase • Excretion of p-HPPA in urine
Case 1 • 2 weeks infant: convulsions, mousy odor in urine, • Ferric chloride test; green
Plasma phenylalanine ↑increased • Urine Phenylalanine, Phenylpyruvate, Phenyllactate ↑
What is the defect? • Why convulsions? • Why fair skin? • What is the importance of early diagnosis?
Case 2 • 3 yrs child is having white hair + fair skin • addition of THB had no effect • What is the biochemical defect? • Will there be any abnormality of catecholamine metabolism?
Case 3 • Mother of 1.5 year old child came with complaint of progressive appearance of hyperchromic papules on his second fingers of both hands since 1 year. he also had darkening of urine & diaper. • What is the diagnosis?
"Once you start a working on something,don't be afraid of failure and don't abandon it. People who work sincerely are the happiest." Chanakya quotes (Indian politician, strategist and writer, 350 BC-275BC)