Download
1 / 1
20 likes | 282 Vues
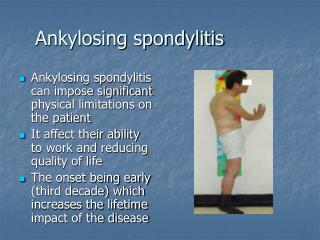
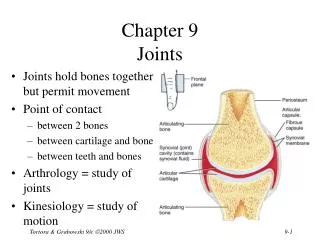
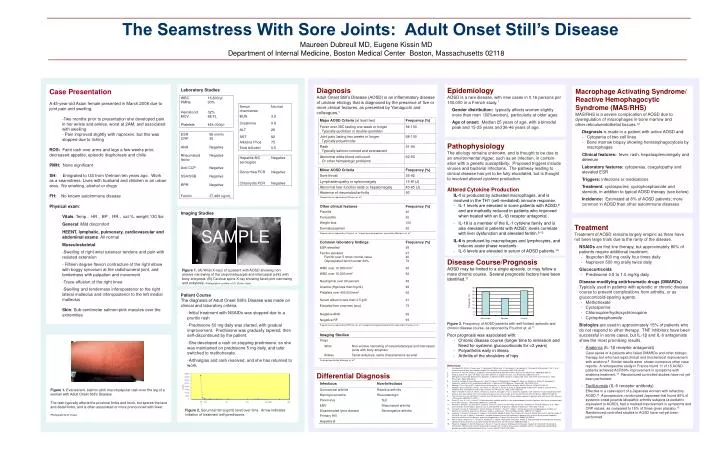
Frequency (%). The Seamstress With Sore Joints: Adult Onset Still’s Disease. Maureen Dubreuil MD, Eugene Kissin MD Department of Internal Medicine, Boston Medical Center Boston, Massachusetts 02118. Diagnosis Adult Onset Still’s Disease (AOSD) is an inflammatory disease

E N D
Frequency (%) The Seamstress With Sore Joints: Adult Onset Still’s Disease Maureen Dubreuil MD, Eugene Kissin MD Department of Internal Medicine, Boston Medical Center Boston, Massachusetts 02118 • Diagnosis • Adult Onset Still’s Disease (AOSD) is an inflammatory disease • of unclear etiology that is diagnosed by the presence of five or • more clinical features, as presented by Yamaguchi and • colleagues.1 • Differential Diagnosis Epidemiology AOSD is a rare disease, with new cases in 0.16 persons per 100,000 in a French study.7 Gender distribution: typically affects women slightly more than men (60%women), particularly at older ages Age of onset: Median 25 years of age, with a bimodal peak and 15-25 years and 36-46 years of age. • Case Presentation • A 45-year-old Asian female presented in March 2008 due to joint pain and swelling. • Two months prior to presentation she developed pain in her wrists and ankles, worst at 2AM, and associated with swelling • Pain improved slightly with naproxen, but this was stopped due to itching • ROS: Faint rash over arms and legs a few weeks prior, decreased appetite, episodic diaphoresis and chills • PMH: None significant • SH: Emigrated to US from Vietnam ten years ago. Work as a seamstress. Lives with husband and children in an urban area. No smoking, alcohol or drugs • FH: No known autoimmune disease • Physical exam: • Vitals: Temp , HR , BP , RR , sat %, weight 130 lbs • General: Mild discomfort • HEENT, lymphatic, pulmonary, cardiovascular and abdominal exams: All normal • Musculoskeletal: • Swelling of right wrist extensor tendons and pain with • resisted extension • Fifteen degree flexion contracture of the right elbow with boggy synovium at the radiohumeral joint, and tenderness with palpation and movement • Trace effusion of the right knee • Swelling and tenderness inferoposterior to the right lateral malleolus and inferoposterior to the left medial malleolus • Skin: Sub-centimeter salmon-pink macules over the extremities • Laboratory Studies • Imaging Studies • Patient Course • The diagnosis of Adult Onset Still’s Disease was made on clinical and laboratory criteria. • Initial treatment with NSAIDs was stopped due to a pruritic rash • Prednisone 50 mg daily was started, with gradual improvement. Prednisone was gradually tapered, then self-discontinued by the patient. • She developed a rash on stopping prednisone, so she was maintained on prednisone 5 mg daily, and later switched to methotrexate. • Arthralgias and rash resolved, and she has returned to work. • Macrophage Activating Syndrome/ • Reactive Hemophagocytic • Syndrome (MAS/RHS) • MAS/RHS is a severe complication of AOSD due to • dysregulation of macrophages in bone marrow and • other reticuloendothelial tissues.12 • Diagnosis is made in a patient with active AOSD and: • Cytopenia of two cell lines • Bone marrow biopsy showing hematophagocytosis by macrophages • Clinical features: fever, rash, hepatosplenomegaly and • delerium • Laboratory features: cytopenias, coagulopathy and • elevated ESR • Triggers: infections or medications • Treatment: cyclosporine, cyclophosphamide and • steroids, in addition to typical AOSD therapy (see below) • Incidence: Estimated at 8% of AOSD patients; more • common in AOSD than other autoimmune diseases • Pathophysiology • The etiology remains unknown, and is thought to be due to • an environmental trigger, such as an infection, in combin- • ation with a genetic susceptibility. Proposed triggers include • viruses and bacterial infections. The pathway leading to • clinical disease has yet to be fully elucidated, but is thought • to involved altered cytokine production. • Altered Cytokine Production • IL-1is produced by activated macrophages, and is • involved in the TH1 (cell-mediated) immune response. • IL-1 levels are elevated in some patients with AOSD,8 and are markedly reduced in patients who improved when treated with an IL-1β receptor antagonist . • IL-18 is a member of the IL-1 cytokine family and is also elevated in patients with AOSD; levels correlate with liver dysfunction and elevated ferritin.9,10 • IL-6 is produced by macrophages and lymphocytes, and induces acute phase reactants. • IL-6 levels are elevated in serum of AOSD patients.14 • Disease Course/Prognosis • AOSD may be limited to a single episode, or may follow a • more chronic course. Several prognostic factors have been • identified.11 • Poor prognosis was associated with: • Chronic disease course (longer time to remission and Need for systemic glucocorticoids for >2 years) • Polyarthritis early in illness • Arthritis of the shoulders of hips • Treatment • Treatment of AOSD remains largely empiric as there have • not been large trials due to the rarity of the disease. • NSAIDs are first line therapy, but approximately 80% of patients require additional treatment. • Ibuprofen 800 mg orally four times daily • Naproxen 500 mg orally twice daily • Glucocorticoids • Prednisone 0.5 to 1.0 mg/kg daily • Disease-modifying antirheumatic drugs (DMARDs) Typically used in patients with episodic or chronic disease course to prevent complications from arthritis, or as glucocorticoid-sparing agents. • Methotrexate • Cyclosporine • Chloroquine/hydroxychloroquine • Cyclophosphamide • Biologics are used in approximately 15% of patients who do not respond to other therapy. TNF inhibitors have been successful in some cases, but IL-1β and IL-6 antagonists show the most promising results. • Anakinra (IL-1β receptor antagonist) • Case series of 4 patients who failed DMARDs and other biologic therapy, but who had rapid clinical and biochemical improvement with anakinra.8 Similar results were shown numerous other case reports. A retrospective study in France found 11 of 15 AOSD patients achieved ACR50% improvement in symptoms with anakinra treatment.13 Randomized controlled studies have not yet been performed. • Tocilizumab (IL-6 receptor antibody) • Effective in a case report of a Japanese woman with refractory AOSD.14 A prospective, randomized Japanese trial found 80% of systemic-onset juvenile idiopathic arthritis subjects (a pediatric equivalent to AOSD), had a marked improvement in symptoms and CRP values, as compared to 15% of those given placebo.15 Randomized controlled studies in AOSD have not yet been performed. SAMPLE A B Figure 1. (A) Wrist X-rays of a patient with AOSD showing non-erosive narrowing of the carpometacarpal and intercarpal joints with bony ankylosis. (B) Cervical spine X-ray showing facet joint narrowing and ankylosis. Radiographs courtesy of Dr. Burton Sack. Figure 3. Frequency of AOSD patients with self-limited, episodic and chronic disease course, as reported by Pouchot et. al.11 • References • Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, Kashiwazaki S, Tanimoto K, Matsumoto Y, Ota T, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol. 1992;19(3):424-30. • Efthimiou P, Paik PK, Bielory L. Diagnosis and management of adult onset Still's disease. Ann Rheum Dis. 2006;65(5):564-72. • Singh S, Samant R, Joshi VR. Adult onset Still's disease: a study of 14 cases. Clin Rheumatol. 2008;27(1):35-9. • Mehrpoor G, Owlia MB, Soleimani H, Ayatollahi J. Adult-onset Still's disease: a report of 28 cases and review of the literature. Mod Rheumatol. 2008;18(5):480-5. • Fautrel B, Le Moël G, Saint-Marcoux B, Taupin P, Vignes S, Rozenberg S, KoegerAC, Meyer O, Guillevin L, Piette JC, Bourgeois P. Diagnostic value of ferritin and glycosylated ferritin in adult onset Still'sdisease.J Rheumatol. 2001;28(2):322-9. • Medsger TA Jr, Christy WC. Carpal arthritis with ankylosis in late onset Still's disease. Arthritis Rheum. 1976;19(2):232-42. • Magadur-Joly G, Billaud E, Barrier JH, Pennec YL, Masson C, Renou P, Prost A. Epidemiology of adult Still's disease: estimate of the incidence by a retrospective study in west France. Ann Rheum Dis. 1995 Jul;54(7):587-90. • Kötter I, Wacker A, Koch S, Henes J, Richter C, Engel A, Günaydin I, Kanz L. Anakinra in patients with treatment-resistant adult-onset Still's disease: four case reports with serial cytokine measurements and a review of the literature.Semin Arthritis Rheum. 2007;37(3):189-97. • Choi JH, Suh CH, Lee YM, Suh YJ, Lee SK, Kim SS, Nahm DH, Park HS. Serum cytokine profiles in patients with adult onset Still's disease. J Rheumatol. 2003;30(11):2422-7. • Chen DY, Lan JL, Lin FJ, Hsieh TY. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset Still's disease. J Rheumatol. 2004;31(11):2189-98. • Pouchot J, Sampalis JS, Beaudet F, Carette S, Décary F, Salusinsky-Sternbach M, Hill RO, Gutkowski A, Harth M, Myhal D, et al. Adult Still's disease: manifestations, disease course, and outcome in 62 patients. Medicine (Baltimore). 1991;70(2):118-36. • Fukaya S, Yasuda S, Hashimoto T, Oku K, Kataoka H, Horita T, Atsumi T, Koike T. Clinical features of haemophagocytic syndrome in patients with systemic autoimmune diseases: analysis of 30 cases. Rheumatology (Oxford). 2008;47(11):1686-91. • Lequerré T, Quartier P, Rosellini D, Alaoui F, De Bandt M, Mejjad O, Kone-Paut I, Michel M, Dernis E, Khellaf M, Limal N, Job-Deslandre C, Fautrel B, Le Loët X, Sibilia J; Interleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in France. Ann Rheum Dis. 2008;67(3):302-8. • Matsumoto K, Nagashima T, Takatori S, Kawahara Y, Yagi M, Iwamoto M, Okazaki H, Minota S. Glucocorticoid and cyclosporine refractory adult onset Still's disease successfully treated with tocilizumab. Clin Rheumatol. 2009;28(4):485-7. • Yokota S, Imagawa T, Mori M, Miyamae T, Aihara Y, Takei S, Iwata N, Umebayashi H, Murata T, Miyoshi M, Tomiita M, Nishimoto N, Kishimoto T. Efficacy and safety of tocilizumab in patients with systemic-onset juvenile idiopathic arthritis: a randomised, double-blind, placebo-controlled, withdrawal phase III trial. Lancet. 2008;371(9617):998-1006. Figure 1. Evanescent, salmon-pink maculopapular rash over the leg of a woman with Adult Onset Still’s Disease. The rash typically affects the proximal limbs and trunk, but spares the face and distal limbs, and is often associated or more pronounced with fever. Photograph by E. Kissin Figure 2. Serum ferritin (ng/ml) level over time. Arrow indicates initiation of treatment with prednisone.