Download

1 / 28
280 likes | 463 Vues
SICU research meeting Hepatocyte growth factor (HGF) and lung transplantation rejuction. Ri 楊勝吉. Case presentation. 08 陳孟婷 23F 4577047 SLE with ARDS s/p bilateral lung transplantation. Bilateral femoral head AVN.

E N D
SICU research meeting Hepatocyte growth factor (HGF)and lung transplantation rejuction Ri楊勝吉
Case presentation • 08 陳孟婷 • 23F 4577047 • SLE with ARDS s/p bilateral lung transplantation. • Bilateral femoral head AVN. • Pulmonary TB s/p complete treatment course on 2002, suspect relapse • Acute respiratory failure, suspect acute rejection
Case presentation • exertional dyspnea, fever, and pleural effusionIntermittent bilateral knee pain • 2002: Open-lung biopsy performed reported interstitial pneumonia while cardiac echogram reported severe pulmonary hypertension • in 2003: pulmonary fibrosis and pulmonary hypertension
Case presentation • 950718: Bil. sequential lung transplantation • 951019: discharge • 9510: dyspnea and cough recentely • 11/3 bronchoscope:no much sputum • 11/4 consult Rehabilitation Add solumedrol • 1106: S/C: TB1107: DC Rifinah, add INAH, Extubation1108 oral intake:fair
Case presentation • CXR(9):improved • WBC: 3.5(5)3.9(6)3.5(7)3.78(8) • CRP:22.7(4)3.94(7)2.26(8) • BUN/cr:6.8/0.9,Cre(U):36 • C0:273(8) • O2mask 35%10L/min • ABG:7.434/36.4/88.9/24.5(9)
Case presentation • Sp/c:TB (11/6), Mycoplasma Ab: Neg • PE: RBC:3000, • WBC: 2600L:N:M+H=21:63:16 • Legionella: (-) S/C: no aerobic pathogen(3) • CMV: positive(1)B/C: no pathogen(3) • Aspergillous Ag: (-)(3) • 24hr CCr: 38Stool WBC: neg, ob: neg • B/S: bil crackles Sputum: 自咳 • Fever subside since 1104
treatment Myambutol(11/02~) INAH(1107~) Solumedrol(11/02~) Cyclosporin(11/03~) Neoral(1103~) Feeding fair
Acute rejection • common in the first weeks • it is often difficult to distinguish acute rejection from infection • Symptoms • malaise, dyspnea, and low-grade fever • Signs are also confusing • falling FEV1, CXR, elevated WBC, hypoxemia, pleural effusion • shotgun treatment Mason: Murray & Nadel's Textbook of Respiratory Medicine, 4th ed., 2005
Acute rejection • Transbronchial biopsy is the gold standard for diagnosis of acute rejection • at least five pieces of tissue • with adequate tissue, the sensitivity: 80%, and the specificity ~100% in the absence of complicating infections Mason: Murray & Nadel's Textbook of Respiratory Medicine, 4th ed., 2005
between acute rejection and infection • cytokine milieu, cellular components in bronchoalveolar lavage fluid, or other local factors (TGF-β mRNA, interferon-γassociated ICAM-1,) • clear distinctions cannot be made without a histologic diagnosis • gene up-regulation(cytokines and chemokines ) Mason: Murray & Nadel's Textbook of Respiratory Medicine, 4th ed., 2005
The literatures • Ross DJ, Moudgil A, Bagga A, et al. Lung allograft dysfunction correlates with gamma-interferon gene expression in bronchoalveolar lavage. J Heart Lung Transplant 1999; 18: 627–36. • Bewig B, Tiroke A, Bottcher H, et al. Adhesion molecules in patients after lung transplantation. Clin Transplant 1999; 13: 432–39. • Khurshid A, Barnett VT, Sekosan M, Schraufnagel DE, Erdö s EG, Deddish P. Carboxypeptidase (CPM) in bronchoalveolar lavage(BAL) fluid of lung transplant recipients. Am J Respir Crit Care Med1998; 157: 811 (abstr). • Bewig B, Stewart S, Bottcher H, et al. Eosinophilic alveolitis in BAL after lung transplantation. Transpl Int 1999; 12: 266–72.
Prediction of lung-transplant rejection by hepatocyte growth factor whether HGF could be an accurate marker for prediction of lung-graft rejection Seyedhossein Aharinejad, Shahrokh Taghavi, Walter Klepetko, Dietmar Abraham, THE LANCET • Vol 363 • May 8, 2004, 1503-1507
Hepatocyte growth factor (HGF) • was first detected in the plasma of partially hepatectomised rats and later purified from human plasma and lung fibroblasts. • Studies in animals suggest that it is a sensitive measure of kidney-graft ejection. Dark JH. Diagnosis of lung rejection.[comment]. [Comment. Journal Article] Lancet. 363(9420):1487-8, 2004 May 8.
109 patient • Serum samples were collected and coded, daily (1st week), every 2 days (w2-w5), then weekly to 24 weeks
Rejection was diagnosed • on the basis of transbronchial lung biopsy, bronchoalveolar lavage, chest radiography, blood-gas analysis, and pulmonary-function tests. (grade A2 or higher) • patients had new radiographic pulmonary opacification and deterioration of blood gases and pulmonary function without evidence of infection at a rejection score.(A0–1 )
treatment • methylprednisolone, 1 g/day intravenously, for 3 days. • improvement of clinical features and a rejection grade of A0 on a subsequent transbronchial lung biopsy sample proved the clinical diagnosis. • OKT3 monoclonal antibody (5 mg/day) for 10 days (steroid resistant patient) • All patients received antiviral prophylaxis.
Assay and Statistical analysis • ELISA for HGF • clinical features and HGF serum concentrations were plotted over time and analysed. • ANOVA was used to compare HGF concentrations in patients before transplantation and in patients with no events at different time points after transplantation.
Assay and Statistical analysis • Spearman’s rank method: Correlations between C-reactive protein concentration, leucocyte count, and HGF concentration • Logistic regression analysis: predictive ability of serum HGF concentrations for lung-graft rejection, in the presence of other potential events that could affect serum HGF concentrations, such as infection. • Statistical analyses used SPSS
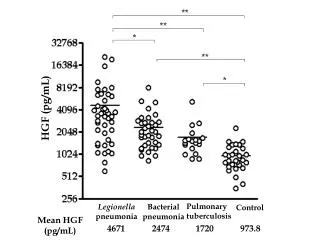
Results • The mean serum HGF concentration was 645 ng/L(SD 259) in controls. • Before transplantation the mean concentration was 1457 ng/L (703) (COPD), 1401 ng/L (572) (CF), and • 1217 ng/L (533) (idiopathic lung fibrosis )(no significant difference); the overall mean in all patients was • 1358 ng/L (603).
The mean serum HGF concentration in these patients increased substantially on the first postoperative day (p<0·0001)
Result • Serum HGF concentration was a significant predictor of rejection (p=0·012). • serum HGF concentration was not a predictor for infection (p=0·852) • Infection (bacterial or fungal; no invasive viral infections were observed in our patients) slightly increased serum HGF concentrations (1559 ng/L [SD 323]) but not significantly compared with patients who had no events or the controls.
Result • In patients with rejection episodes, there was no significant correlation between serum C-reactive protein and HGF concentrations (rs=-0·085; p=0·688) or between leucocyte count and HGF concentrations (rs=0·372; p=0·067).
Discussion • Serum HGF concentrations rise in fulminant hepatitis and in patients with inflammatory lung diseases. • rejection might involve a wider range of mediators, the processes of growth and remodelling, which are closely associated with chronic rejection. • support the hypothesis that HGF is a pulmotrophic substance, and its serum concentrations could be associated with the degree of lung injury and repair. Mal H, Dehoux M, Sleiman C, et al. Early release of proinflammatory cytokines after lung transplantation. Chest 1998; 113:645–51.
discussion • HGF concentrations returned to near preoperative values after steroid therapy, which supports a mechanistic link with steroids. • The lack of correlation with serum markers of inflammation in this and previous studies suggests that the change in HGF is not related directly to inflammatory or acute-phase reactions • combined antiviral prophylaxis we used could explain the absence of invasive viral and cytomegalovirus infections in our patients Tsubouchi H, Niitani Y, Hirono S, et al. Levels of the human hepatocyte growth factor in serum of patients with various liver diseases determined by an enzyme-linked immunosorbent assay. Hepatology 1991; 13: 1–5.
discussion • HGF was produced by mesenchymal cells in each organ, which might regulate epithelial cell growth and organ morphogenesis in a paracrine or endocrine way (macrophages, fibroblasts, and endothelial cells) • reperfusion injury and endothelial- cell production of HGF. Defrances MC, Wolf HK, Michalopoulos GK, Zarnegar R. The presence of hepatocyte growth factor in the developing rat. Development 1992; 116: 387–95. Matsumoto K, Tajima H, Hamanoue M, Kohno S, Kinoshita T, Nakamura T. Identification and characterization of “injurin,” an inducer of expression of the gene for hepatocyte growth factor. Proc Natl Acad Sci USA 1992; 89: 3800–04.
discussion • fibroblasts become activated during the early repair stages of bronchial and vascular anastomoses. • HGF stimulates the proliferation of lung epithelial cells and HGF might have an important role in proliferation of bronchial epithelium Maeda J, Ueki N, Hada T, Higashino K. Elevated serum hepatocyte growth factor/scatter factor levels in inflammatory lung disease.Am J Respir Crit Care Med 1995; 152: 1587–91.
Conclusion • graft rejection but not infection results in an early significant rise in HGF concentrations and that the values decline after steroid treatment suggest that HGF could be a sensitive predictor of lung graft rejection.
Comment • There is no information about correlations with early performance of the lung • Despite the correlation between early rejection and bronchiolitis obliterans syndrome (BOS), no one has shown clearly that reduction in rejection rates has a positive benefit on the prevalence of the syndrome. • If early treatment of rising levels of hepatic growth factor, before significant airway injury occurs reduces the incidence of BOS, Aharinejad and colleagues will have made a real contribution to the major clinical problem in lung transplantation. Dark JH. Diagnosis of lung rejection.[comment]. [Comment. Journal Article] Lancet. 363(9420):1487-8, 2004 May 8.
![cu'jf ;|f] ts ] Gb|,dGynL ,/ fd ]5fk](https://cdn1.slideserve.com/2425388/slide1-dt.jpg)