Download
1 / 46
1.25k likes | 3.38k Vues
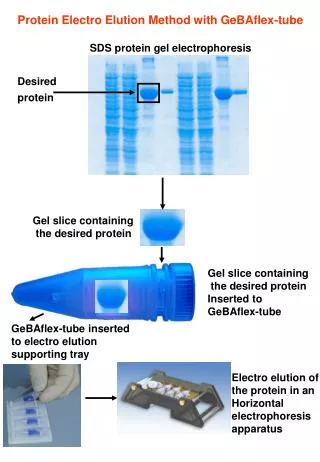
Serum Protein Electrophoresis with Immunofixation. Dr.Ajay Phadke Centre Head SRL Diagnostics- Dr.Avinash Phadke’s Lab. What is electrophoresis?. Electrophoresis is a method of separating proteins based on their physical properties .

E N D
Serum Protein Electrophoresis with Immunofixation Dr.AjayPhadke Centre Head SRL Diagnostics-Dr.AvinashPhadke’s Lab
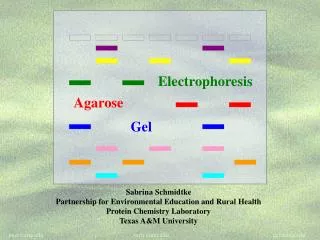
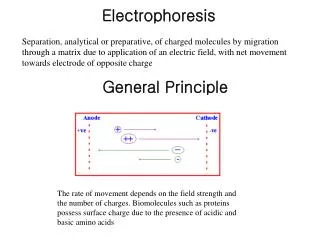
What is electrophoresis? • Electrophoresis is a method of separating proteins based on their physical properties. • Proteins can be separated using a buffered solid medium (agarose electrophoresis ) or using only the liquid phase (capillary electrophoresis) • The net charge (positive or negative) and the size and shape of the protein commonly are used in differentiating various serum proteins. • A negatively charged particle usually travels to the positively charged electrode(Gel EP) • In Capillary EP ? Negatively charged particle travels to the negatively charged electrode(Cathode) • WHY?
Capillary Electrophoresis in Minicap/Capillarys Anode + Cathode - DETECTION OF PROTEINS INJECTION OF SERUM Protein migration EOF Electro migration Positive charges of the buffer solution The Electro-Osmotic Flow (EOF) is a stronger force than the Electrical Field. As a result, all proteins are carriedtowards the cathodic end of the capillary. Negative charges of capillarywall
The complementary positively charged ions in the surrounding buffer are free to move under the electromotive force, and they carry with them molecules of the solvent water. • This buffer flow is termed electro-osmosis or endosmosis, which also carries the proteins with it to some extent by mechanical flow, not by charge. • The actual distance traveled by a particular protein migrating in an electrical field is determined by the elec- tromotive force (a feature of the protein itself and the pH) and the electro- osmotic force (a function primarily of the support medium). • When the electro-osmotic force is greater than the electrophoretic force acting on weakly anionic proteins (e.g., γ-globulins), those proteins move from the application point toward the cathode, even though their charge is slightly negative.
Electrophoretic System in Minicap/Capillarys Capillarys Electrophoresis Principle Thermic bridge Temperature Controlled by Peltier device Migration Capillary in thermo-conductive resin Detector Deuterium lamp High Voltage Cathode - Anode +
When do doctors ask for SPE? • Unexplained anemia / weakness / fatigue / ↑ ESR • Unexplained renal insufficiency • Heavy proteinuria in patient >40yrs • BenceJones proteinuria • Hypercalcaemia • Hypergammaglobulinemia • Immunoglobulin deficiency • Peripheral neuropathy (5% will have MGUS) • Recurrent infections • Unexplained bone pain / pathologic fracture / lytic lesion-
1.Elderly patient with suspicion for MM i.e bone pain, lytic lesion • 2. fever for >1 month • 3. ESR increase, persistent anemia, fatigue • 4. CRP high • 5.Heavy proteinuria in adults • 6.persistent increase in calcium • 7.Peripheral neuropathy since a percentage have MGUS
Capillarys 2 Minicap
Carousel 28 positions
Reagent Compartment Easy access to consumables:reagent cups, waste & reagents containers (2 buffer vials on board)
Fraction identification Albumin Beta-1 Alpha-1 Alpha-2 Beta-2 Gamma a-1 acidglycoprotein a-1 antitrypsin TBG, Transcortin Gammaglobulins C3 complement B Lipoprotein Haptoglobin Hemopexin Transferrin a-2 macroglobulin Ceruloplasmin
Normal Gaussian aspect in gamma & No increase or additional deformation/peak in gamma, beta 1, beta 2 and alpha 2 a2 b2 Alb g a1 b1
Albumin • Albumin concentrations are vital to the understanding and interpretation of calcium and magnesium levels because these ions are bound to albumin, and so decreases in albumin are directly responsible for depression of their concentrations
C3 (and also C4) concentration is a convenient marker for assessing disease activity in rheumatic disorders such as lupus erythematosus and rheumatoid arthritis. • C4 is not appreciated on serum protein electrophoresis because its concentration is normally only about one-fifth that of C3. • Both C3 and C4 are now easily quantitated by nephelometry for monitoring rheumatic disease activity
Monoclonal peak in Gamma a2 b2 Alb g a1 b1
Monoclonal peak in beta a2 b2 Alb g a1 b1
Oligoclonal pattern a2 b2 Alb g a1 b1
Immunofixation & immunotyping • Principle: Apply the patients sample on gel. Separate the sample. Add antibody . If positive = on washing this sample remains because of large size of complex. • Immunotyping : similar principle. Automated, not labour intensive. • BASIC DIFFERENCE: way how sample is processed. WE MIX sample with antibody before processing.Complex is made EVEN BEFORE SEPERATION TAKES PLACE. Then injected into capillary. Monoclonal complex will MIGRATE SLOWLY and will NOT form a peak. • THEREFORE, in IF you are looking for the band to be PRESENT. While in IT you are looking for it to be ABSENT! • IFE is Very labour intensive
IEP: serum applied to aggelin wells. EP . Antisera added. 24 hr incubation. ARCS formed • IFE:Sample on solid matrix • IT: NO GEL. Migration in buffered medium. Mono-specific antisera. REDUCTION technique. Antisera binds to Immunoglobulin. Heavy, large molecule created. Pulled OUT of viewing area. • If PEAK DETECTEd, just click on immunotyping after selecting dilution. • Hypgogamma : Ig<0.8g/L(1/10) • Std :Ig 0.8- 2.0 g/L(1/20) • Hypergamma: Ig >2.0g/L(1/40)
Monoclonal peak or polyclonal increase in gamma? Pointedpeak Rounded top Narrow basement Large basement Polyclonalincrease Monoclonal peak IT IT Complete substractionwith the antiserumagainst a heavychain and partial substractionwith the antiseraagainst kappa and lambda Complete substraction of the peakwith one antiserumagainst a heavychain and a light chain
The peak disappears in Ig G Abnormal peak in gamma The peak disappears in Kappa Conclusion: Detection of monoclonal Ig G Kappa
Wheninterpreting IT, alwaysconsider: « If removingsomething, whatisremaining? » In eachwindow, removing one specific class of IgGhighlightswhatishappening with the residualimmunoglobulinsthatremainaftersubstraction
Hints and tips for IT interpretation • Examine carefully all IT curves without a zoom to verify the correct overlapping on albumin and the zone of interest between ELP and antisera curves • Verify that the correct sample dilution has been used • Compare the residual heavy and light chains after substraction and their position to verify additional presence of other monoclonal Ig • If there is no correspondence between heavy and light chains, complete the test with an immunofixation to check for free light chains and/or IgD, IgE
When does one advise urine EP • The following conditions (to list a few) warrant urine protein electrophoresis: 1) monoclonal protein in serum is >1.5 g/dL, 2) monoclonal free light chains are detected in serum, 3) hypogammaglobulinemia is present in serum; 4) serum electrophoresis shows nephrotic pattern. • “In the context of screening, the serum FLC assay in combination with serum protein electrophoresis (PEL) and immunofixation yields high sensitivity, and negates the need for 24-h urine studies for diagnoses other than light chain amyloidosis (AL).” • • “...once diagnosis of a plasma cell disorder is made, 24-h urine studies are required for all patients.” • • “For AL screening, however, the urine IFE should still be done in addition to the serum tests including the serum FLC.” • • “The FLC assay cannot replace the 24-h urine protein electrophoresis for monitoring myeloma patients with measurable urinary M proteins”.
What history is important? What would you report?
Increase in alpha1, alpha 2 Advise renal profile,UPE and IT
65 year old patient. Weakness, What do you see on the graph. What will you advise?
50 year old female What is your impression? What would you advise?
30 Year old Female. What is your opinion? What history will you take
Hb: 8.0 • RDW: 20.3 • Retic N • Ferritin : 3.0 Normal range(4.6-204) • B 12 : 254