Download
1 / 47
470 likes | 489 Vues
This research focuses on developing a hierarchical symmetry-based automatic stroke detection framework for brain CT scans at all stages of pathology. By utilizing innovative techniques like wavelet decomposition and modified Metropolis dynamics, the system aims to differentiate between hemorrhagic, chronic, normal, acute, and hyperacute strokes. The study underscores the importance of early and accurate stroke detection to facilitate timely treatment decisions.

E N D
Analysis of Stroke on Brain Computed Tomography Scans Saurabh Sharma 200502024 Adviser: Prof. Jayanthi Sivaswamy 4rd October 2013
Outline • Introduction • Problem Description • Part I : • Automatic detection of stroke • Part II : • Contrast enhancement of stroke tissues • Region based • Pixel based • Conclusions • Future Directions
Introduction • Stroke, a.k.a cerebrovascular accident is loss of brain function due to disturbance in blood supply. 15 Million people are affected from stroke worldwide.
Introduction • Stroke, a.k.acerebrovascular accident is loss of brain function due to disturbance in blood supply. • Stoke can be: Hemorrhagic Ischemic
Introduction • Both the hemorrhage and ischemic stroke are fatal in nature. • Complete recovery possible in hemorrhage but less so in case of ischemic stroke • Most of the damage in case of ischemic stroke occurs within four hours of onset. • Each hour of untreated stroke ages the brain by ~3.6 years.
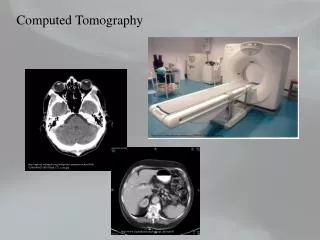
Treatment • Hemorrhage and ischemic stroke have conflicting treatments. • Physiological changes in hemorrhage can be detected much earlier than stroke. • Lack of tissue information in CT, cannot detect ischemic stroke in most cases before the damage is done. • The golden rule is first use CT to rule out hemorrhage and then go for MRI to detect ischemic stroke.
Why choose CT? • CT imaging is relatively quick, provides better spatial resolution • CT is more widely available than MR scanners in developing countries • Cost differential between CT and MRI scans • Moreover, if infarct can be detected at the first scan ( CT ) itself then it would save valuable time
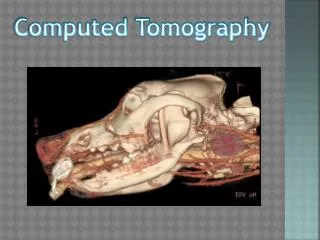
Problem Statement • To aid in detection of stroke from brain CT scans during all stages of pathology. Hemorrhage Chronic Normal Acute Hyperacute
Track 1 • Hierarchical symmetry based automatic stroke detection framework. • Stroke is characterized as an aberration in the otherwise symmetrical distribution of tissues between the left and right hemispheres.
Preprocessing • Mid-Sagittal plane detection and rotation correction. • Most of the existing methods used tissue symmetry or center of mass based solutions. • We devised a novel technique making use of physical structure of the nose to detect the rotation angle.
Level 1 Classification • Quantize the histograms of both the hemispheres into 5 bins, 0-50, 50 -100,…,200-250 • Compare the 50-100 and the 200-250 bins from the left and right hemispheres. • If the dissimilarity observed is greater than a particular threshold assign the case to hemorrhage to chronic (50-100) , hemorrhage (200-250) and normal* (otherwise) bins.
Level 2 Classification • Need for a finer symmetry comparison to sort out the acute from the normal + hyperacute cases. • Wavelet decomposition of the histogram is done and the energy distribution is computed up to 5 levels in scale-space. • A threshold value, computed empirically, is then used to separate out the acute cases based on the energy values.
Level 3 Classification • At hyperacute stage, very subtle changes take place in the affected tissues. • Most of these changes (~2-3 gray scale levels) are very difficult to identify. • As a result, we turn to some of the specific signs demonstrated by hyperacute infarct.
Level 3 Classification • The best bet : detect the blurring of gray \ white matter. • Difficult to achieve in case of CT imaging due to the image quality, noise etc. • We propose using a rough segmentation of the brain tissues into gray \ white matter to determine the presence of stroke. Rough segmentation image.
Level 3 Classification MRF based Tissue Segmentation Skull based Symmetry detection Infarct Decision Candidate Selection Wavelet based Image Enhancement Input CT Image
Level 3 Classification Wavelet based Image Enhancement • The input CT image is first striped of the skull. • In the next step, the input image is subjected to SVD based image contrast enhancement technique proposed by Demirel et al*. *H. Demirel, C. Ozcinar, and G. Anbarjafari. Satellite image contrast enhancement using discrete wavelet transform and singular value decomposition. IEEE GRS Letters, 7(2):333 –337, april 2010.
Level 3 Classification MRF - MAP based Tissue Segmentation Where, L is a random variable denoting the class and S is the site location (x,y) Assuming I.I.D Gaussian distribution at each location
Level 3 Classification MRF - MAP based Tissue Segmentation • To obtain the final mappings, we iteratively find the configuration which has the lowest energy. • The method employed is called Modified Metropolis Dynamics (MMD) as it is generally faster and provides a lower energy output. M. Berthod, Z. Kato, S. Yu, and J. Zerubia. Bayesian image classification using markov random-fields. Image and Vision Computing, 14(4):285–295,May 1996.
Level 3 Classification Candidate Selection Infarct Decision • Weed out false positives using size and confidence constraints
Qualitative Results Pre Processed Input Image Rough Segmentation Final Result
Qualitative Results Input Image Preprocessed Final Output Follow – up
Quantitative Results Dataset Details. • The dataset contains 42 volume CT scans. • Out of 42, we have 19 normal, 5 hemorrhagic and 6 each of chronic, acute and hyperacute. • In addition, we have the follow up scans of the hyperacute cases. • For robust testing, the test data was collected from a wide range of age groups. (7, 15, 20 datasets in age groups 0-30, 30-50, 50 and above respectively)
Track 2 • Enhancement of Early Infarct through Auto-Windowing • Early automatic detection difficult. • Current detection process used by doctors. • Issues with existing tissue contrast enhancement techniques. • Propose a novel auto-windowing technique which aims at finding the windowing setting which maximizes the contrast between the normal and stroke affected tissues.
Manual Windowing • The process of mapping the 16-bit CT image to the 8-bit display monitors.
Manual Windowing • The process of mapping the 16-bit CT image to the 8-bit display monitors. • Can bring about either contrast stretching or compression.
Manual Windowing • Stroke under different window settings.
Auto Windowing • We propose two different approaches for auto windowing. Pixel based Region based
Auto Windowing • We propose two different approaches for auto windowing. • Use the automatic detection of Track 1 to identify the window settings. • Plot the histograms of the stroke affected tissues and their counter-parts in the other hemisphere. • Find the gray scale value which best separates the two histograms and use this as the window center. • Now choose any window width based on how much tissue information is required. Pixel based Region based
Auto Windowing • We propose two different approaches for auto windowing. Pixel based Region based
Auto Windowing • We propose two different approaches for auto windowing. Pixel based Region based
Auto Windowing • We propose two different approaches for auto windowing. • Inspired by binary thresholding mechanism • The optimum window setting is defined as one which maximizes the difference in distribution of pixels in the left and right hemispheres. • Operation is carried out on two separate images, left and right hemisphere, unlike one in case of thresholding. • Several techniques exist but difficult to model two image problem using those techniques. Pixel based Region based
Auto Windowing • We propose two different approaches for auto windowing. • We modeled our two-image thresholding on the parzen window based thresholding proposed by wang et al. • Parzen window is a technique to estimate the probability density P(x, y) at a point (x, y). Pixel based Region based S.Wang, F. lai Chung, and F. Xiong. A novel image thresholding method based on parzen window estimate. Pattern Recognition, 41(1):117 – 129, 2008
Auto Windowing • We propose two different approaches for auto windowing. Pixel based Region based Ωland Ωrare the set of pixels in left and right hemispherical image
Auto Windowing • We propose two different approaches for auto windowing. Pixel based Region based
Qualitative Results Experiment Details • A set of 15 slices each of hyperacute and normal cases were selected • The slices were shown to the radiologists under normal, region-based (Wr) and pixel-based (Wp) automated window settings. • Each slice by rated by 4 radiologists, of varied experience, in a blinded review for the presence of hyperacute infarct. • Their response and the time taken for decision was recorded.
Qualitative Results • Average sensitivity increased from 59.95% (Ws) to 79.97% (Wr) and 84.97% (Wp). (P = 0.034 for Wp, P = 0.040 for Wr) • Average specificity increased from 83.3% (Ws) to 98.34% (Wr) and 98.34 % (Wp). (P = 0.032 for Wr) • Overall accuracy of the radiologists increased from 71% (Ws) to 91.6% (Wp, p = 0.024) and 89.16% (Wr, p = 0.034) • The performance of younger radiologists show much more improvement though still not statistically significant.
Summary • Presented an unified hierarchical approach for automatic detection and classification of stroke. • Our approach models the stroke as a disturbance in the otherwise similar distribution of brain tissue with respect to the mid-sagittal plane • The method gives very good recall and sensitivity on hemorrhage, chronic and acute stroke and appreciable performance on hyperacute or early infarct. • The hyperacute infarct detection can be used to aid the radiologists in clinical environment.
Summary • We also presented an auto-windowing approach to aid the radiologists in detection of early infarct. • The perception experiment results show that auto-windowing approach could be applied in clinical settings. • The method also hinted at bridging the experience divide by bringing the accuracy of inexperienced radiologists to a very good level.
Future Directions • Application to similar problems where early detection of diseases is difficult. • One such case is the early detection of brain tumors. • Need to test on a larger dataset.